- Infectious Diseases of Livestock
- Part 3
- Clostridium perfringens type B infections
- GENERAL INTRODUCTION: SPIROCHAETES
- Swine dysentery
- Borrelia theileri infection
- Borrelia suilla infection
- Lyme disease in livestock
- Leptospirosis
- GENERAL INTRODUCTION: AEROBIC ⁄ MICRO-AEROPHILIC, MOTILE, HELICAL ⁄ VIBROID GRAM-NEGATIVE BACTERIA
- Genital campylobacteriosis in cattle
- Proliferative enteropathies of pigs
- Campylobacter jejuni infection
- GENERAL INTRODUCTION: GRAM-NEGATIVE AEROBIC OR CAPNOPHILIC RODS AND COCCI
- Moraxella spp. infections
- Bordetella bronchiseptica infections
- Pseudomonas spp. infections
- Glanders
- Melioidosis
- Brucella spp. infections
- Bovine brucellosis
- Brucella ovis infection
- Brucella melitensis infection
- Brucella suis infection
- Brucella infections in terrestrial wildlife
- GENERAL INTRODUCTION: FACULTATIVELY ANAEROBIC GRAM NEGATIVE RODS
- Klebsiella spp. infections
- Escherichia coli infections
- Salmonella spp. infections
- Bovine salmonellosis
- Ovine and caprine salmonellosis
- Porcine salmonellosis
- Equine salmonellosis
- Yersinia spp. infections
- Haemophilus and Histophilus spp. infections
- Haemophilus parasuis infection
- Histophilus somni disease complex in cattle
- Actinobacillus spp. infections
- Actinobacillus equuli infections
- Gram-negative pleomorphic infections: Actinobacillus seminis, Histophilus ovis and Histophilus somni
- Porcine pleuropneumonia
- Actinobacillus suis infections
- Pasteurella and Mannheimia spp. infections
- Pneumonic mannheimiosis and pasteurellosis of cattle
- Haemorrhagic septicaemia
- Pasteurellosis in sheep and goats
- Porcine pasteurellosis
- Progressive atrophic rhinitis
- GENERAL INTRODUCTION: ANAEROBIC GRAM-NEGATIVE, IRREGULAR RODS
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: GRAM-POSITIVE COCCI
- Staphylococcus spp. infections
- Staphylococcus aureus infections
- Exudative epidermitis
- Other Staphylococcus spp. infections
- Streptococcus spp. infections
- Strangles
- Streptococcus suis infections
- Streptococcus porcinus infections
- Other Streptococcus spp. infections
- GENERAL INTRODUCTION: ENDOSPORE-FORMING GRAM-POSITIVE RODS AND COCCI
- Anthrax
- Clostridium perfringens group infections
- Clostridium perfringens type A infections
- Clostridium perfringens type B infections
- Clostridium perfringens type C infections
- Clostridium perfringens type D infections
- Malignant oedema⁄gas gangrene group of Clostridium spp.
- Clostridium chauvoei infections
- Clostridium novyi infections
- Clostridium septicum infections
- Other clostridial infections
- Tetanus
- Botulism
- GENERAL INTRODUCTION: REGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Listeriosis
- Erysipelothrix rhusiopathiae infections
- GENERAL INTRODUCTION: IRREGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Corynebacterium pseudotuberculosis infections
- Corynebacterium renale group infections
- Bolo disease
- Actinomyces bovis infections
- Trueperella pyogenes infections
- Actinobaculum suis infections
- Actinomyces hyovaginalis infections
- GENERAL INTRODUCTION: MYCOBACTERIA
- Tuberculosis
- Paratuberculosis
- GENERAL INTRODUCTION: ACTINOMYCETES
- Nocardiosis
- Rhodococcus equi infections
- Dermatophilosis
- GENERAL INTRODUCTION: MOLLICUTES
- Contagious bovine pleuropneumonia
- Contagious caprine pleuropneumonia
- Mycoplasmal pneumonia of pigs
- Mycoplasmal polyserositis and arthritis of pigs
- Mycoplasmal arthritis of pigs
- Bovine genital mycoplasmosis
- Neurotoxin-producing group of Clostridium spp.
- Contagious equine metritis
- Tyzzer's disease
- MYCOTIC AND ALGAL DISEASES: Mycoses
- MYCOTIC AND ALGAL DISEASES: Pneumocystosis
- MYCOTIC AND ALGAL DISEASES: Protothecosis and other algal diseases
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Epivag
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ulcerative balanoposthitis and vulvovaginitis of sheep
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ill thrift
- Eperythrozoonosis
- Bovine haemobartonellosis
Clostridium perfringens type B infections
This content is distributed under the following licence: Attribution-NonCommercial CC BY-NC  View Creative Commons Licence details here
View Creative Commons Licence details here

Clostridium perfringens type B infections
Synonym: Lamb dysentery
Previous authors:
N P J KRIEK, M Q ODENDAAL AND P HUNTER
Current authors:
F A UZAL - Professor and Branch Chief, DVM, FRVC, MSc, PhD, Dipl. ACVP, California Animal Health and Food Safety Lab, University of California, Davis, San Bernardino, California, 92408, USA.
M NAVARRO - Assistant Professor of Veterinary Anatomic Pathology, DVM, MSc, PhD, Dipl. ACVP, Universidad Austral de Chile, Campus Isla Teja, Valdivia, Chile.
N P J KRIEK - Emeritus Professor, BVSc, MMed Vet (Path), Onderstepoort, Pretoria, Gauteng, 0110, South Africa.
P HUNTER-OBEREM - Self Employed, BVSc Hons, Mont Lorraine, Gauteng, South Africa.
Introduction
Infection by Clostridium perfringens type B causes a peracute, acute, subacute or chronic enterotoxaemia in lambs that is also occasionally encountered in goat kids and calves, and rarely in foals. The disease occurs mainly in countries in the Middle East and Europe.22 The infection has not been reported in the Americas, although anecdotal evidence suggests that cases may have occurred in this region.
In lambs, the disease is also known as lamb dysentery and it usually affects those that are younger than 14 days. It is characterized clinically by an acute, haemorrhagic to mucohaemorrhagic diarrhoea, and rarely, by neurologic signs. Lambs die after a few hours to two days in the peracute and acute cases, and after four or more days in the subacute and chronic cases.5, 12, 17, 21
Aetiology
The organism grows in the intestinal tract of affected animals where it produces the toxins responsible for the disease. Clostridium perfringens type B encodes alpha, beta and epsilon toxins, and a number of other, usually referred to as minor, toxins.3 The beta and epsilon toxins are metabolic products secreted during the exponential growth phase of C. perfringens type B in a suitable environment that contains the nutrients required for toxin production. Beta toxin is encoded in a plasmid14 and its concentration in the growth medium in vitro declines rapidly after prolonged incubation.3
For information on the cultural, morphological and biochemical characteristics of C. perfringens and its toxins, refer to the introductory chapter: Clostridium perfringens group infections.
Epidemiology
Although heavier breeds and crossbreeds are considered to be more resistant, lamb dysentery affects new-born lambs of all sheep breeds to the same extent. Goat kids are also affected, albeit less frequently, and information on the disease in this species is scant.4 In sheep, the disease seems to be more prevalent during cold weather, while it is rare in autumn, and it does not appear to occur in summer.4
Clostridium perfringens type B is excreted in the faeces of adult carrier animals and sick lambs, thereby contaminating soil and pastures. Although there is little scientific evidence to support this claim,15 it is thought that C. perfringens type B strains only survive for several months in soil and pastures, and they are also not considered to be part of the normal microbial flora of the soil. The teats of ewes become contaminated with faeces and soil, and their lambs acquire the infection per os while suckling.4 It has been suggested that lambs are more prone to develop the disease on certain parts of a farm, mainly those where ewes and lambs are confined to small areas. Close and prolonged confinement of sheep seem to increase the severity of the disease. The prevalence of the disease decreases when the ewes and lambs are removed from highly contaminated areas.
Pathogenesis
Clostridium perfringens type B organisms ingested within the first few hours after birth of the lambs, colonize the intestines, in all likelihood especially the small intestine, where they multiply and produce their toxins that act both locally and are absorbed into the general circulation.
The potent and lethal beta and epsilon toxins are the main virulence factors of C. perfringens type B,13 and they are, respectively, highly trypsin-sensitive, and fully dependent on trypsin for full activation. Although there is no evidence to substantiate it, it has been suggested that only one of the toxins is involved in the pathogenesis of C. perfringens type B disease at any given time.3 It is believed that the beta toxin is primarily responsible for the induction of the intestinal lesions characteristic of type B enterotoxaemia. The role of epsilon toxin in this condition is poorly understood but it is assumed to be responsible for the lesions (focal symmetrical encephalomalacia) in the central nervous system (CNS) in the a few cases of type B enterotoxaemia in which such lesions have been recorded.3
The toxins are produced in vitro during the exponential growth phase of C. perfringens, and it is assumed that the same pertains to their in vivo growth.3 Restriction of the occurrence of the disease to neonates is, as in the case of C. perfringens type C infections, thought to be due to the blocking effect of colostrum on trypsin and other proteases, as these enzymes are powerful beta-toxin inhibitors. The trypsin-blocking effect of colostrum is thought to be an evolutionary trait to protect colostral immunoglobulins from trypsin break-down.14, 22 In older animals these enzymes are not inhibited and remain in the intestinal lumen in sufficient quantities to inactivate beta toxin.18 In the portions of the small, and, to a lesser extent the large intestine, where the toxins are produced, multifocal to diffuse necrosis and damage to the vascular network develop that cause a malabsorptive diarrhoea.19 The consequent loss of water and electrolytes, especially HCO3, results in severe dehydration and acidosis. Death is the combined result of shock, toxaemia, dehydration, and acidosis.7
Clinical signs
Lamb dysentery is almost exclusively a disease of neonatal lambs, with rare cases occurring in other species.22 One-to-seven-day-old animals are the most severely affected. The disease usually first appears towards the end of the lambing season in a sheep-breeding unit. During subsequent breeding seasons, however, outbreaks usually commence 14 days after the first ewes have lambed.
When outbreaks initially occur on a farm, lambs of 1- to 3-days-old are affected, but during subsequent years older lambs of up to two to three weeks of age may also contract the disease. The morbidity is 20 to 30 per cent with an expected 100 per cent lethality.7, 15, 19, 22
The incubation period varies from 12 hours to two days, and clinical signs are often present within 24 hours of birth.17, 21 Lamb dysentery may have a peracute, acute, subacute, chronic or mild course.7, 22 Peracutely affected lambs usually die without manifesting any clinical signs. The course of the acute and subacute disease may extend over one or more days while, in the chronic disease, lambs survive longer than three or four days. Older animals become increasingly resistant; those older than 14 days are only mildly affected and they rarely die.19
Acutely affected lambs are weak, listless, and suckle sluggishly or refuse to do so and they may show evidence of abdominal pain and diarrhoea, the faeces becoming brownish-grey, semi-liquid and bloodstained, and they soon become comatose and die. Subacutely affected lambs are dull, listless and depressed, move about sluggishly, lag behind the rest of the flock, often lie down, and are reluctant to stand up and suckle. If they do get up, or when lifted to their feet, they stretch in a peculiar way, in that they may remain standing for a while with their backs arched, obviously in pain. Abdominal pain, bleating and diarrhoea are commonly manifested. foul-smelling faeces are at first yellow and semi-liquid and then become mucus-coated, dark and bloodstained, and are passed with the animals straining severely. A yellow, blood-tinged, faecal discharge caked around the tail base, may be evident. Lambs eventually become prostrate, comatose and die.11, 12, 21, 22 The chronic disease is characterized by listlessness and unthriftiness. The lambs suckle listlessly and seldom drink enough milk to maintain their basic requirements. They frequently lie down and, on rising, stretch their backs in a peculiar way. Their faeces are thin, mucoid and bloodstained.22
Non-specific neurological signs, including opisthotonus, have been reported in all three forms of the disease.3, 12, 22
Clostridium perfringens type B enterotoxaemia has been reported, albeit rarely, in calves and foals but information available about the disease in these species is scant.5, 10, 11 Cases of the disease were reported in seven-to ten-day-old calves, characterized mainly by scouring.5, 11 In the few cases of the disease described in foals, mortality rates of up to 50 per cent have been recorded. The clinical signs included cessation of suckling, pain and a severe, haemorrhagic diarrhoea that developed within 48 hours after birth. In fatal cases, the foals became comatose and they died within 12 to 24 hours after first becoming ill.10
Pathology
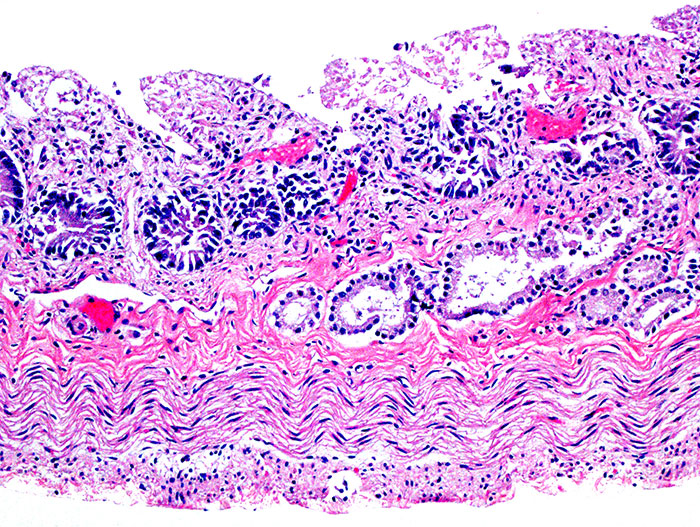
In lambs, rare cases of C. perfringens type B infection may present without macroscopic lesions.21, 22 The intestinal lesions taht occur predominantly in the ileum, are similar to the necrotizing enteritis caused by C. perfringens type C. They are characterized by a severe, diffuse or multifocal to coalescing, necro-haemorrhagic and/or ulcerative enteritis, accompanied by a haemorrhagic intestinal content (Figures 1 and 2). In the disease with a more protracted clinical course, little or no haemorrhage may be present in the intestinal tract. In most cases, a clear serous or haemorrhagic fluid is present in the peritoneal cavity. Perforation of the intestinal wall causing a fibrinous peritonitis that can lead to intestinal adhesions, may also be seen occasionally.12, 19, 21, 22

Extra-intestinal lesions are those characteristic of toxaemia and include congested and oedematous lungs, a pale or congested, friable liver, splenomegaly due to congestion, hydropericardium (Figure 3) and, epicardial and endocardial haemorrhages. Focal symmetrical encephalomalacia (FSE), macro- and microscopically identical to that seen in chronic cases of C. perfringens type D enterotoxaemia, has been described in a few cases.3

The macroscopic lesions in the gastrointestinal tract of calves and foals with C. perfringens type B infection are very similar to those described in lambs.10, 22 No macroscopic lesions have been described in the CNS of these two species.
Diagnosis
Based on clinical signs, and the macro- and microscopic lesions, a presumptive diagnosis of C. perfringens type B enterotoxaemia can be made. While small numbers of C. perfringens type B have rarely been isolated from the intestinal contents of normal animals in some areas of the world, isolation of large numbers of the bacterium from individuals with compatible macro- and microscopic lesions, is supportive of a diagnosis of C. perfringens type B infection.12, 22 A final, confirmed diagnosis, however, should be based on the presence of both beta and epsilon toxins in the intestinal content of affected animals. Currently, ELISA is the method of choice for their detection and there are several ELISAs that detect both toxins in the same panel.9, 21 Failure to detect beta toxin does not rule out C. perfringens type B as a cause, because this toxin is highly trypsin-sensitive and is rapidly broken down soon after its production in the intestine.14 Therefore, a final diagnosis of C. perfringens type B infection should not be based on toxin detection alone, because if beta toxin has been destroyed by intestinal proteases, such infection may be misdiagnosed as type D (in which alpha and epsilon toxins are produced).13 Clinical, pathological and microbiological findings should always be appraised in association with toxin detection when attempting to confirm the diagnosis.16, 21
Differential diagnosis
Lamb dysentery may be confused with the acute, fatal, neonatal diarrhoea caused by enterotoxigenic Escherichia coli K99 (F5) from which it can be distinguished by the absence of the macro- and microscopical mucosal lesions that are characteristic of lamb dysentery.19 Necrotic enteritis caused by C. perfringens type C presents with almost identical macro- and microscopic lesions to lamb dysentery, and differentiation should be based on toxin detection and the results of anaerobic culture.18, 19
Control
Most lambs cannot be successfully treated when suffering from the peracute or acute disease, but the use of antibiotics administered orally together with supportive treatment can save mildly affected lambs. C. perfringens is resistant to the aminoglycoside group of antibiotics, but susceptible to chloramphenicol, and penicillin (for further detail refer to the introductory chapter: Clostridium perfringens group infections. The treatment of the remaining lambs in an outbreak with anti-type B-specific immunoglobulin, if it is available, may be beneficial.20, 21
During an outbreak of the disease, it is important to isolate affected lambs (and their dams) as soon as possible. The healthy animals in the breeding flock should immediately be removed to other areas where ewes have not previously lambed, as pens and paddocks that have housed infected lambs may be severely contaminated and serve as a source of infection. It is important that the lambs ingest colostrum within the first two to six hours of life.20
To control anticipated or subsequent outbreaks of the disease, pregnant ewes should be immunized to induce the presence of as high a level of protective antibodies in the colostrum as possible, as the passive transfer of maternal immunity to lambs is the only way to protect them from becoming infected during the first days of life.20, 21 Pregnant ewes vaccinated for the first time, should receive two injections four to six weeks apart, the second injection being scheduled to be administered four to eight weeks before lambing.6, 20, 22 Ewes that were previously immunized, require a single booster vaccination two to four weeks before the expected commencement of parturition in the ensuing lambing seasons. Polyvalent clostridial vaccines containing several different antigens, including C. perfringens type B toxoid, are available in many countries.1, 6, 8, 21 Most commercially available C. perfringens type B vaccines consist of an alum-precipitated toxoid of the epsilon and beta toxins.2
Legend to figures
Figure 1. Distended and diffusely hyperaemic small intestine in a lamb with Clostridium perfringens type B enterotoxaemia. Photo courtesy John Munday.
Figure 2. Necrotic small intestine in a lamb with Clostridium perfringens type B enterotoxaemia. H&E stain.
Figure 3. Hydropericardium with fibrin clots in a lamb with Clostridium perfringens type B enterotoxaemia. Photo courtesy John Munday.
References
- ARDEHALI, M. & DARAKHSHAN, H., 1976. Production and standardization of polyvalent Clostridium perfringens vaccine in Iran. Development in Biological Standardization, 32, 31–34.
- ERASMUS, B. J., CAMERON, C. M., HUNTER, P., CILLIERS, J. A., OBEREM, P. T., STOLTSZ, W. H. & DE WAAL, D. T., 1990. Onderstepoort Vaccines Booklet issued by the Department of Agriculture and Development and obtainable from the Directorate of Agricultural Information, Private Bag X144, Pretoria 0001.
- FERNANDEZ-MIYAKAWA, M. E., FISHER, D. J., POON, R., SAYEED, S., ADAMS, V., ROOD, J. I., MCCLANE, B. A. & UZAL, F. A., 2007. Both epsilon-toxin and beta-toxin are important for the lethal properties of Clostridium perfringens type B isolates in the mouse intravenous injection model. Infection and Immunity, 75, 1443-1452.
- HENNING, M. W., 1956. Animal Diseases in South Africa. 3rd edn. Pretoria, South Africa: Central News Agency Ltd.
- HEPPLE, J. R., 1952. Necrotic enterotoxaemia in a calf due to Clostridium welchii type B. Veterinary Record, 64, 633-634.
- JANSEN, B. C., 1976. The standardization of C. perfringens antigens and antisera. Development in Biological Standardization, 32, 35-44.
- JENSEN, R. & SWIFT, B. L., 1982. Diseases of Sheep, 2nd edition. Philadelphia, Lea & Febiger.
- KERRY, J. B. & CRAIG, G. R., 1979. Field studies in sheep with multicomponent clostridial vaccines. Veterinary Record, 105, 551-554.
- MARTIN, P. K., NAYLOR, R. D. & SHARPE, R. T., 1988. Detection of Clostridium perfringens β toxin by enzyme-linked immunosorbent assay. Research in Veterinary Science, 44(2), 270-271.
- MASON, J. H. & ROBINSON, E. M., 1938. The isolation of Cl. welchii type B from foals affected with dysentery. Onderstepoort Journal of Veterinary Science and Animal Industry, 11, 333-337.
- MONTGOMERIE, R. F., 1961. Clostridium perfringens (Cl. welchii) enterotoxaemia in the ruminant. Canadian Veterinary Journal, 2, 439-450.
- MUNDAY, J. S., BENTALL, H., ABERDEIN, D., NAVARRO, M., UZAL, F. A. & BROWN, S. T., 2020. Death of a neonatal lamb due to Clostridium perfringens type B in New Zealand. New Zealand Veterinary Journal, 68(4), 242-246.
- ROOD, J. I., ADAMS, V., LACEY, J., LYRAS, D., MCCLANE, B. A., MELVILLE, S. B., MOORE, R. J., POPOFF, M. R., SARKER, M. R., SONGER, J. G. & UZAL, F. A., 2018. Expansion of the Clostridium perfringens toxin-based typing scheme. Anaerobe, 53, 5-10.
- SAYEED, S., UZAL, F. A., FISHER, D. J., SAPUTO, J., VIDAL, J. E., CHEN, Y., GUPTA, P., ROOD, J. I. & MCCLANE, B. A., 2008. Beta toxin is essential for the intestinal virulence of Clostridium perfringens type C disease isolate CN3685 in a rabbit ileal loop model. Molecular Microbiology, 67(1), 15-30.
- SMITH, L. D. S. & WILLIAMS, B. L., 1984. The Pathogenic Anaerobic Bacteria. 3rd edition, Springfield, Illinois: Charles C. Thomas.
- STERNE, M. & BATTY, I., 1975. Pathogenic Clostridia. London, Boston, Butterworths.
- UZAL, F. A., 2004. Diagnosis of Clostridium perfringens intestinal infections in sheep and goats. Anaerobe, 10(2), 135-143.
- UZAL, F. A. & MCCLANE, B. A., 2011. Recent progress in understanding the pathogenesis of Clostridium perfringens type C infections. Veterinary Microbiology, 153(1-2), 37-43.
- UZAL, F. A., PLATTNER, B. L. & HOSTETTER, J. M., 2016. Diseases of the alimentary system. In: Pathology of Domestic Animals. G. Maxie (ed), 6th edition. Elsevier, St. Louis, MO, 1-257.
- UZAL, F. A. & SMITH, B. P., 2019. Clostridium perfringens type B. In: Large Animal Internal Medicine. SMITH, B. P., VAN METRE, D. C. & PUSTERLA, N., (eds.), 6th edition Elsevier, St. Louis, MO, 900-901.
- UZAL, F. A. & SONGER, J. G., 2008. Diagnosis of Clostridium perfringens intestinal infections in sheep and goats. Journal of Veterinary Diagnostic Investigation, 20(3), 253-265.
- UZAL, F. A. & SONGER, J. G., 2016. Infections by Clostridium perfringens type B. In: Clostridial Diseases of Animals. UZAL, F. A., SONGER, J. G., PRESCOTT, J. F. & POPOFF, M. R., (eds.). Wiley Blackwell, Ames, IA, 139-142.




