- Infectious Diseases of Livestock
- Part 3
- Glanders
- GENERAL INTRODUCTION: SPIROCHAETES
- Swine dysentery
- Borrelia theileri infection
- Borrelia suilla infection
- Lyme disease in livestock
- Leptospirosis
- GENERAL INTRODUCTION: AEROBIC ⁄ MICRO-AEROPHILIC, MOTILE, HELICAL ⁄ VIBROID GRAM-NEGATIVE BACTERIA
- Genital campylobacteriosis in cattle
- Proliferative enteropathies of pigs
- Campylobacter jejuni infection
- GENERAL INTRODUCTION: GRAM-NEGATIVE AEROBIC OR CAPNOPHILIC RODS AND COCCI
- Moraxella spp. infections
- Bordetella bronchiseptica infections
- Pseudomonas spp. infections
- Glanders
- Melioidosis
- Brucella spp. infections
- Bovine brucellosis
- Brucella ovis infection
- Brucella melitensis infection
- Brucella suis infection
- Brucella infections in terrestrial wildlife
- GENERAL INTRODUCTION: FACULTATIVELY ANAEROBIC GRAM NEGATIVE RODS
- Klebsiella spp. infections
- Escherichia coli infections
- Salmonella spp. infections
- Bovine salmonellosis
- Ovine and caprine salmonellosis
- Porcine salmonellosis
- Equine salmonellosis
- Yersinia spp. infections
- Haemophilus and Histophilus spp. infections
- Haemophilus parasuis infection
- Histophilus somni disease complex in cattle
- Actinobacillus spp. infections
- Actinobacillus equuli infections
- Gram-negative pleomorphic infections: Actinobacillus seminis, Histophilus ovis and Histophilus somni
- Porcine pleuropneumonia
- Actinobacillus suis infections
- Pasteurella and Mannheimia spp. infections
- Pneumonic mannheimiosis and pasteurellosis of cattle
- Haemorrhagic septicaemia
- Pasteurellosis in sheep and goats
- Porcine pasteurellosis
- Progressive atrophic rhinitis
- GENERAL INTRODUCTION: ANAEROBIC GRAM-NEGATIVE, IRREGULAR RODS
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: GRAM-POSITIVE COCCI
- Staphylococcus spp. infections
- Staphylococcus aureus infections
- Exudative epidermitis
- Other Staphylococcus spp. infections
- Streptococcus spp. infections
- Strangles
- Streptococcus suis infections
- Streptococcus porcinus infections
- Other Streptococcus spp. infections
- GENERAL INTRODUCTION: ENDOSPORE-FORMING GRAM-POSITIVE RODS AND COCCI
- Anthrax
- Clostridium perfringens group infections
- Clostridium perfringens type A infections
- Clostridium perfringens type B infections
- Clostridium perfringens type C infections
- Clostridium perfringens type D infections
- Malignant oedema⁄gas gangrene group of Clostridium spp.
- Clostridium chauvoei infections
- Clostridium novyi infections
- Clostridium septicum infections
- Other clostridial infections
- Tetanus
- Botulism
- GENERAL INTRODUCTION: REGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Listeriosis
- Erysipelothrix rhusiopathiae infections
- GENERAL INTRODUCTION: IRREGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Corynebacterium pseudotuberculosis infections
- Corynebacterium renale group infections
- Bolo disease
- Actinomyces bovis infections
- Trueperella pyogenes infections
- Actinobaculum suis infections
- Actinomyces hyovaginalis infections
- GENERAL INTRODUCTION: MYCOBACTERIA
- Tuberculosis
- Paratuberculosis
- GENERAL INTRODUCTION: ACTINOMYCETES
- Nocardiosis
- Rhodococcus equi infections
- Dermatophilosis
- GENERAL INTRODUCTION: MOLLICUTES
- Contagious bovine pleuropneumonia
- Contagious caprine pleuropneumonia
- Mycoplasmal pneumonia of pigs
- Mycoplasmal polyserositis and arthritis of pigs
- Mycoplasmal arthritis of pigs
- Bovine genital mycoplasmosis
- Neurotoxin-producing group of Clostridium spp.
- Contagious equine metritis
- Tyzzer's disease
- MYCOTIC AND ALGAL DISEASES: Mycoses
- MYCOTIC AND ALGAL DISEASES: Pneumocystosis
- MYCOTIC AND ALGAL DISEASES: Protothecosis and other algal diseases
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Epivag
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ulcerative balanoposthitis and vulvovaginitis of sheep
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ill thrift
- Eperythrozoonosis
- Bovine haemobartonellosis
Glanders
This content is distributed under the following licence: Attribution-NonCommercial CC BY-NC  View Creative Commons Licence details here
View Creative Commons Licence details here

Glanders
J J VAN DER LUGT AND G C BISHOP*
Introduction
Glanders is a contagious disease primarily of solipeds caused by the bacterium Burkholderia mallei. It is characterized by nodules, ulcers and the formation of scars, particularly in the upper respiratory tract, lungs, skin, and less frequently in other organs. It may occur in an acute or chronic form, is usually fatal and is of major importance in any infected equine population. Glanders once occurred extensively throughout the world, including South Africa. At present it occurs only sporadically in eastern European countries, North Africa,14 and Asia (including India,16 Iran,4 Pakistan,15 Turkey1 and China12). It is a zoonosis.
Glanders was already recognized in 400 BC by Hippocrates, and a century later by Aristotle.8, 9 The bacterium was first isolated by Loeffler and Schütz in 1882, but it was only four years later that Loeffler demonstrated beyond doubt that it was the cause of glanders. During 1891 and 1892, no less than seven European scientists died of the disease following accidental laboratory infection.8
Glanders was spread by animal movements through trade or war to most countries of the world.8 Henning9 expressed uncertainty about the way in which it was introduced into South Africa, but in his review of the disease, Hunting8 mentions that during the Anglo-Boer War (1899 to 1902), in which 240 000 horses perished, South Africa was plagued by the spread of glanders throughout the entire country. According to Hunting, the disease was introduced into South Africa by remounts imported from the UK, America and Australia, and possibly also from Europe. Eventually, in 1929, glanders was restricted to the Cape Peninsula, from which it was eradicated soon afterwards by application of a slaughter-out policy (Figure 142.1 and Figure 142.2). This control measure and the use of the mallein test for diagnostic purposes were the major reasons for the successful eradication of the disease.
Glanders is unlikely to assume any great significance in southern Africa unless the pathogen is reintroduced under circumstances where large numbers of horses or other solipeds are kept under unsanitary conditions.
Aetiology
Burkholderia mallei (syn. Pseudomonas mallei, Actinobacillus mallei, Malleomyces mallei and Pfeifferella mallei) is a Gram-negative, non-motile, non-encapsulated and nonspore- forming bacillus5 which is obligately aerobic (except in media containing nitrate), is nutritionally versatile and does not require special growth factors. The best growth of B. mallei is obtained at 37 °C. Potato media are particularly suited for its cultivation.9 In vitro DNA hybridization experiments suggest a close relationship to B. pseudomallei, the causative organism of false glanders or melioidosis (see Melioidosis).
The bacterium is not very resistant against external factors. It is destroyed by exposure to direct sunlight within 24 hours and is killed by most of the common disinfectants, e.g. phenol, potassium permanganate, copper sulphate, formalin and chlorine. In damp media the organism retains its vitality for three to five weeks and in decomposing material for 20 to 30 days. It may survive for about 20 days in clean water and for about six weeks in contaminated stables.9, 14
Little is known about the virulence factors of B. mallei. A recent study demonstrated that capsular polysaccharide is a major virulence factor and the capsule may prevent efficient clearance of the bacterium by the host immune system.6
Epidemiology
Underfed animals and those kept under unhygienic environments are more susceptible than animals that are healthy and well-cared for. Humans are also highly susceptible; the disease sometimes affects laboratory workers, veterinarians, horse caretakers and slaughterhouse employees who are in intimate contact with affected horses or the organism.
The natural disease occurs primarily in domestic equids and only occasionally in carnivores, rodents, cattle, sheep, goats, pigs and humans.13, 14 All species of domestic equids are highly susceptible. Donkeys are apparently the most susceptible and frequently develop the acute form of the disease.9 Horses are more resistant and commonly contract the chronic form. Mules occupy an intermediate position.
In acute glanders, the pathogen may be distributed throughout the body, whereas in chronic cases the organism appears to be confined to the affected organs and exudates from lesions. Although the urine, saliva, tears and faeces may be contaminated, nasal discharges and the pus from cutaneous ulcers are the most infective. The mode of infection is unclear, but it generally appears to result from contaminated food or water. Outbreaks of the disease are usually favoured where several animals are kept together and share feeding places and water troughs. The occurrence of glanders in lions in an Italian zoological park was traced back to contaminated meat originating from horses which were imported.3, 9


Figure 142.1 and 142.2 Historic photographs depicting mass slaughter of a herd of horses and burning of carcasses during the glanders eradication campaign in the 1920s in South Africa
The frequency of lung involvement has led to the speculation that aerogenous infection is important, yet most attempts to produce chronic glanders via the respiratory tract have failed. Typical glanders, however, has been reproduced by intranasal and intratracheal injections and by feeding the animals infective material.
Cutaneous glanders, also referred to as farcy, occurs as a result of infection of the skin following injury, or from metastases of pulmonary origin.
The importance of asymptomatic carriers, and the transmission of the disease from them to healthy animals, should be emphasized. This form of transmission is considered to be more significant than that from clinical cases.9 Once the disease has been introduced into a stable or a stud it spreads rapidly.
Pathogenesis
Infection taking place per os results in the acute form and is characterized by a septicaemia or bacteraemia.9, 14 Localization in the lungs invariably occurs and, in some cases, also in the skin and nasal mucosa. Nodules may also develop in organs such as the liver, spleen and testes.9 In some animals nodular lesions appear to be the only sign of lung involvement while in others, there may be a bronchopneumonia.9, 14
Clinical signs
Following experimental infection, the incubation period varies according to the route and intensity of infection, and the natural resistance of the animal.9 A fever appears after about three days and clinical signs after a week. Following natural infection, several weeks (and on average, two months) often elapse before the first signs are noticeable.9
In acute glanders there is a high fever, nasal discharge and coughing and swelling of the submandibular lymph nodes.2, 9, 14 The nasal discharge, which is usually unilateral, may be yellowish-green or bloody and may partly accumulate around the nostrils. Nasal mucous membranes are swollen, may be covered by a diphtheritic exudate and contain several nodules which often eventually ulcerate. The ulcers may coalesce; their borders are raised and irregular, and their bases are covered by yellowish granulation tissue. Peculiar rattling and roaring sounds may be heard during breathing. The superficial lymph nodes are swollen and sensitive, and may rupture to discharge a viscous, purulent exudate. Death due to septicaemia occurs within a week or two.
Chronic glanders is more common in horses than the acute form, particularly in countries where the disease is endemic.9, 13, 14 This form may have a duration of years and can be so mild that it is easily overlooked. Intermittent and irregular exacerbations are associated with coughing and dyspnoea. Sometimes the submandibular lymph nodes adhere to the skin and the mandible, and they may be hard and knotty. The extremities, particularly the hind legs, are in some cases severely affected and thickened.
The pulmonary form of glanders may take several months to develop, and culminates in fits of coughing or in a dry persistent cough. Respiration becomes costo-sternal and laboured. Eventually, typical lesions also appear in the nasal mucous membranes and skin.
Nasal glanders usually commences with a unilateral nasal catarrh that becomes progressively more severe, and is eventually characterized by a purulent and greenishyellow nasal discharge sometimes containing streaks of blood or flakes of epithelium. Large quantities of exudate may be expelled during fits of coughing and snorting. Yellowish-grey nodules develop in the nasal mucosa and when the covering epithelium sloughs, these give rise to ulcers with well-defined borders. Healed ulcers leave distinct, stellate scars. The submandibular lymph nodes are initially swollen and painful, but eventually they become firm and less painful and they adhere to the mandible and surrounding skin.
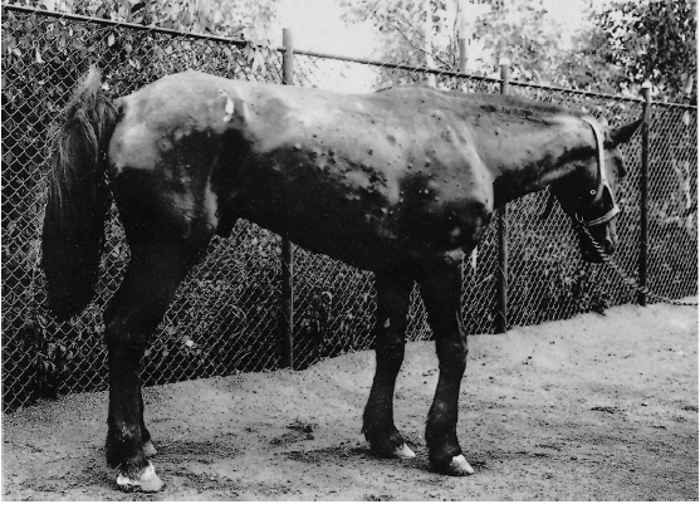
The nodules which develop in the skin and subcutaneous tissue (cutaneous glanders or farcy), particularly of the limbs, sides of the chest and ventral abdomen, may be 10mm in diameter (Figure 142.3). On rupturing, these nodules become ulcers that may heal or spread to the surrounding tissue. Involvement of the lymphatic system is manifested by the presence of inflamed lymphatics which are thickened, nodular and cord-like. They often link nodules and ulcers to each other and the resultant lesions resemble strings of beads. Oedematous swelling of the legs can be so extensive that it interferes with movement.

Pathology
In the acute form, multiple petechiae are found throughout the body, while a severe catarrhal bronchopneumonia and enlargement of the bronchial lymph nodes are typical.
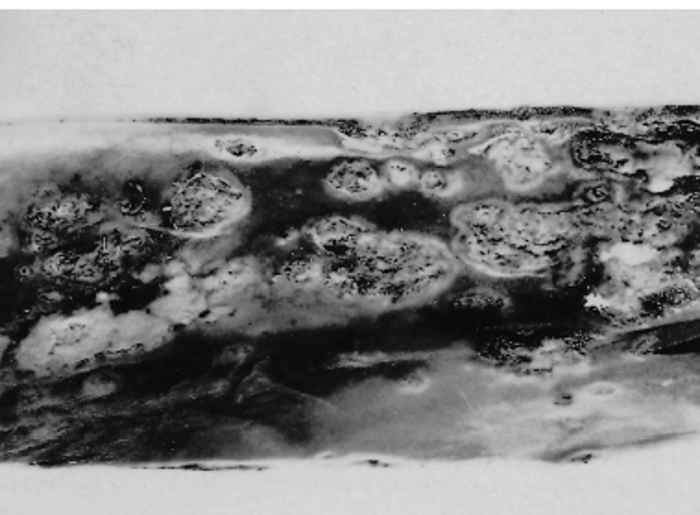
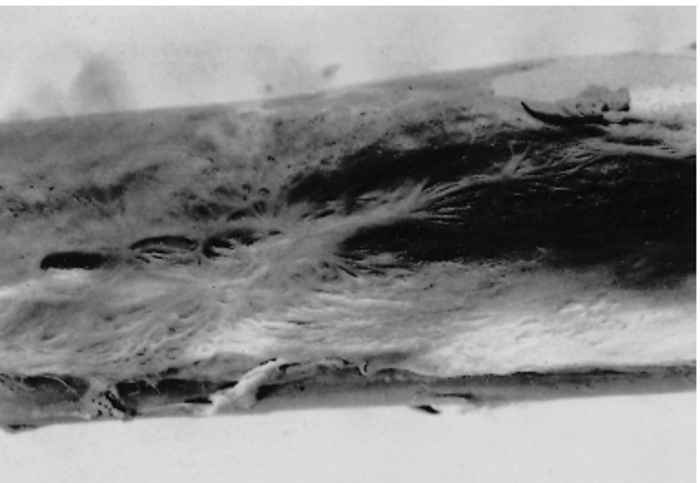
In the more common chronic form, lesions are invariably present in the lungs and palpation reveals nodules resembling tubercles, or areas of bronchopneumonia (Figure 142.4). The nodules are firm, round, encapsulated and greyish. 9, 13, 14 Nodules and ulcers are frequently present in the upper respiratory tract, especially in the nasal septum (Figure 142.5), larynx and trachea. Some of the ulcers may have healed to form bulging or flat, stellate scars (Figure 142.6). Lymph nodes draining affected skin or deep-seated lesions are enlarged. Nodules similar to those in the lung may also be seen in the liver, spleen and kidney.
Lesions in the digestive system are rare. Occasionally lesions from the upper respiratory tract may extend into the pharyngeal mucous membrane.
Microscopically, the nodules are necrogranulomatous and are characterized by necrosis and liquefaction, and at a later stage by caseation and mineralization of their centres. These changes are surrounded by a mixture of inflammatory cells comprising many neutrophils, a few lymphocytes, macrophages, epithelioid cells, and a few giant cells. The nodule is well encapsulated. Vasculitis and thrombosis of the vessels immediately adjacent to the necrotic nodules are prominent features. Circumscribed, haemorrhagic foci are sometimes found in the lung and these may be infiltrated by many neutrophils and a few macrophages.8, 9, 13
The disease is accompanied by anaemia, a leukocytosis and neutrophilia.13
Diagnosis
The characteristic clinical signs of glanders appear late in the course of the disease and a definite diagnosis based on the clinical manifestation alone is seldom possible.9 The mallein or complement fixation (CF) tests should be used to detect the occult or carrier cases, which are very important in the control of the disease.7, 9, 14 The administration of mallein (a solution containing endo- and exotoxins of B. mallei), using the ophthalmic and subcutaneous routes,9 has been largely replaced by the intradermal-palpebral test in which mallein is injected into the lower eyelid of the animal. In positive cases, a delayed hypersensitivity reaction, which is detectable after 48 hours, is responsible for the development of a mucopurulent ocular discharge and marked oedema of the eyelid. Certain strains of the bacterium may, however, cross-react with B. pseudomallei.14 The sensitivity of the mallein test, the indirect haemagglutination test, the CF test and counter-immunoelectrophoresis (CIE) have been compared by using serum samples obtained from 155 horses and 57 mules in India.10 Although it was concluded that CIE is the most rapid, simple and economical test for dealing with large numbers of serum samples, the CF test is the most reliable serological test available. Recent results indicate that the intrapalpebral mallein test may cause uninfected horses and ponies to produce antibodies against B. mallei, causing positive CF tests for glanders.7 A competitive enzyme-linked immunosorbent assay (cELISA)11 and a dot ELISA17 were developed and may replace the current CF test.
Glanders may be confirmed by the bacteriological examination of swabs taken of pus from open lesions.13 The organism grows readily on blood agar, Loeffler’s serum agar or glycerine-potato media incubated aerobically at 37 °C. Colonies are about 1 mm in diameter, white, semitransparent and viscid.
The intraperitoneal injection of infective material into guinea pigs results in death in 10 to 14 days.13 The organism localizes in lymph nodes and on the tunica of the testes, producing a purulent exudate and causing swelling of the scrotum in two to three days.9 This characteristic response is referred to as the Strauss reaction.
Differential diagnosis
Several conditions may be confused with glanders and laboratory examination is essential in differentiating the disease from strangles, ulcerative lymphangitis, botriomycosis, horsepox and such fungal conditions as sporotrichosis caused by Sporothrix schenkii, epizootic lymphangitis caused by Histoplasma farciminosum and ulcerative lymphangitis caused by Corynebacterium pseudotuberculosis.
Control
Treatment with sulphadiazine alone or in combination with formalized preparations of B. mallei has sometimes been successful. Most countries of the western world—including South Africa in which it is a notifiable disease—provide for the slaughter of clinical cases and animals which show a reaction to the mallein test or to one of the serological tests.9 Carcases must be burnt or buried and thorough disinfection of the premises should be undertaken. Complete quarantine of affected and surrounding premises is necessary and equine traffic should be carefully monitored.
Horses may recover spontaneously from the disease, but their subsequent immunity is incomplete. It is not surprising, therefore, that immunization has never been considered successful in the control of the disease.
References
- ALIBASOGLU, M., YESILDERE, T., CALISLAR, T., INAL, T. & CALISKAN, U., 1986. Outbreak of glanders in lions in the Istanbul zoological garden. Berliner und Münchener Tierärzliche Wochenschrift, 99, 57–63.
- ARUN, S., NEUBAUER, H., GÜREL, A., AYYILDIZ, G., KUSÇU, T., YESILDERE, T., MEYER, H. & HERMANUS, W., 1999. Equine glanders in Turkey. The Veterinary Record, 144, 225–258.
- BATTELLI, C., CONTENTO, F., CORSALINI, T., GOFFREDO, G., LAZARI, P., PUCCINI, V. & SOBRERO, L., 1973. Glanders in a group of lions in captivity. Veterinaria Italiana, 24, 87–112, 113–116.
- BAZARGANI, T.T., TADJBAKHSH, H., BADII, A. & ZAHRAEI, T., 1996. The outbreak of glanders in some racehorses in three states of Iran. Journal of Equine Veterinary Science, 16, 232–236.
- BUCHANAN, R.E. & GIBBONS, N.E., 1974. Bergey’s Manual of Determinative Bacteriology. 8th edn. Baltimore: The Williams & Wilkins Co.
- DESHAZER, D., WAAG, D.M., FRITZ, D.L. & WOODS, D.E., 2001. Identification of a Burkholderia mallei polysaccharide gene cluster by subtractive hybridization and demonstration that the encoded capsule is an essential virulence determinant. Microbial Pathogenesis, 30, 253–269.
- HAGEBOCK, J.M., SCHLATER, L.K., FRERICHS, W.M. & OLSON, D.P., 1993. Serologic responses to the mallein test for glanders in solipeds. Journal of Veterinary Diagnostic Investigation, 5, 97–99.
- HUNTING, W., 1913. Glanders. In: hoare, e.w., (ed). A System of Veterinary Medicine. London: Ballière, Tindall and Cox.
- HENNING, M.W., 1956. Animal Diseases in South Africa. 3rd edn. South Africa: Central News Agency Ltd.
- JANA, A.M., GUPTA, A.K., PANDYA, G., VERMA, R.D. & RAO, K.M., 1982. Rapid diagnosis of glanders in equines by counter-immunoelectrophoresis. Indian Veterinary Journal, 59, 5–9.
- KATZ, J., DEWALD, R. & NICHOLSON, J., 2000. Procedurally similar competitive immunoassay systems for the serodiagnosis of Babesia equi, Babesia caballi, Trypanosoma equiperdum and Burkholderia mallei. Journal of Veterinary Diagnostic Investigation, 12, 46–50.
- LIANG, S.Y., WEI, J.S., MEI, W.H., XIE, X., DUAN, X.W. & GONG, R.X., 1980. Post-infection immunity after recovery from glanders. Collected Papers of Veterinary Research, 6, 77–82.
- MACAULAY, J.W., 1978. Glanders. In: french, e.l. & geering, w.a., (eds). Exotic Diseases of Animals: A Manual for Diagnosis. 2nd edn. Canberra: Australian Government Publishing Service.
- RADOSTITS, O.M., GAY, C.C., BLOOD, D.C. & HINCHCLIFF, K.W., 2000. Veterinary Medicine. 9th edn. London: W.B. Saunders Company Ltd.
- VAID, M.Y., MUNEER, M.A. & NAEEM, M., 1981. Studies on the incidence of glanders in Lahore. Pakistan Veterinary Journal, 1, 75.
- VERMA, R.D., 1981. Glanders in India with special reference to incidence and epidemiology. Indian Veterinary Journal, 58, 177–183.
- VERMA, R.D., SHARMA, J.K., VENKATESWARAN, K.S. & BATRA, H.V., 1990. Development of an avidin-biotin dot enzyme-linked immunosorbent assay and its comparison with other serological tests for the diagnosis of glanders in equines. Veterinary Microbiology, 25, 77–85.
- YABUUCHI, E., KOSAKO, Y., OYAIZU, H., HOTTA, H., HASHIMOTO, Y., EZAKI, T. & ARAKAWA, M., 1992. Proposal of Burkholderia gen. nov. and transfer of seven species of the genus Pseudomonas homology group II to the new genus, with the type species Burkholderia cepacia
(Palleroni and Holmes 1981) comb. nov. Microbiology and Immunology, 36, 1251–1275.




