- Infectious Diseases of Livestock
- Part 3
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: SPIROCHAETES
- Swine dysentery
- Borrelia theileri infection
- Borrelia suilla infection
- Lyme disease in livestock
- Leptospirosis
- GENERAL INTRODUCTION: AEROBIC ⁄ MICRO-AEROPHILIC, MOTILE, HELICAL ⁄ VIBROID GRAM-NEGATIVE BACTERIA
- Genital campylobacteriosis in cattle
- Proliferative enteropathies of pigs
- Campylobacter jejuni infection
- GENERAL INTRODUCTION: GRAM-NEGATIVE AEROBIC OR CAPNOPHILIC RODS AND COCCI
- Moraxella spp. infections
- Bordetella bronchiseptica infections
- Pseudomonas spp. infections
- Glanders
- Melioidosis
- Brucella spp. infections
- Bovine brucellosis
- Brucella ovis infection
- Brucella melitensis infection
- Brucella suis infection
- Brucella infections in terrestrial wildlife
- GENERAL INTRODUCTION: FACULTATIVELY ANAEROBIC GRAM NEGATIVE RODS
- Klebsiella spp. infections
- Escherichia coli infections
- Salmonella spp. infections
- Bovine salmonellosis
- Ovine and caprine salmonellosis
- Porcine salmonellosis
- Equine salmonellosis
- Yersinia spp. infections
- Haemophilus and Histophilus spp. infections
- Haemophilus parasuis infection
- Histophilus somni disease complex in cattle
- Actinobacillus spp. infections
- Actinobacillus equuli infections
- Gram-negative pleomorphic infections: Actinobacillus seminis, Histophilus ovis and Histophilus somni
- Porcine pleuropneumonia
- Actinobacillus suis infections
- Pasteurella and Mannheimia spp. infections
- Pneumonic mannheimiosis and pasteurellosis of cattle
- Haemorrhagic septicaemia
- Pasteurellosis in sheep and goats
- Porcine pasteurellosis
- Progressive atrophic rhinitis
- GENERAL INTRODUCTION: ANAEROBIC GRAM-NEGATIVE, IRREGULAR RODS
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: GRAM-POSITIVE COCCI
- Staphylococcus spp. infections
- Staphylococcus aureus infections
- Exudative epidermitis
- Other Staphylococcus spp. infections
- Streptococcus spp. infections
- Strangles
- Streptococcus suis infections
- Streptococcus porcinus infections
- Other Streptococcus spp. infections
- GENERAL INTRODUCTION: ENDOSPORE-FORMING GRAM-POSITIVE RODS AND COCCI
- Anthrax
- Clostridium perfringens group infections
- Clostridium perfringens type A infections
- Clostridium perfringens type B infections
- Clostridium perfringens type C infections
- Clostridium perfringens type D infections
- Malignant oedema⁄gas gangrene group of Clostridium spp.
- Clostridium chauvoei infections
- Clostridium novyi infections
- Clostridium septicum infections
- Other clostridial infections
- Tetanus
- Botulism
- GENERAL INTRODUCTION: REGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Listeriosis
- Erysipelothrix rhusiopathiae infections
- GENERAL INTRODUCTION: IRREGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Corynebacterium pseudotuberculosis infections
- Corynebacterium renale group infections
- Bolo disease
- Actinomyces bovis infections
- Trueperella pyogenes infections
- Actinobaculum suis infections
- Actinomyces hyovaginalis infections
- GENERAL INTRODUCTION: MYCOBACTERIA
- Tuberculosis
- Paratuberculosis
- GENERAL INTRODUCTION: ACTINOMYCETES
- Nocardiosis
- Rhodococcus equi infections
- Dermatophilosis
- GENERAL INTRODUCTION: MOLLICUTES
- Contagious bovine pleuropneumonia
- Contagious caprine pleuropneumonia
- Mycoplasmal pneumonia of pigs
- Mycoplasmal polyserositis and arthritis of pigs
- Mycoplasmal arthritis of pigs
- Bovine genital mycoplasmosis
- Neurotoxin-producing group of Clostridium spp.
- Contagious equine metritis
- Tyzzer's disease
- MYCOTIC AND ALGAL DISEASES: Mycoses
- MYCOTIC AND ALGAL DISEASES: Pneumocystosis
- MYCOTIC AND ALGAL DISEASES: Protothecosis and other algal diseases
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Epivag
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ulcerative balanoposthitis and vulvovaginitis of sheep
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ill thrift
- Eperythrozoonosis
- Bovine haemobartonellosis
Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
This content is distributed under the following licence: Attribution-NonCommercial CC BY-NC  View Creative Commons Licence details here
View Creative Commons Licence details here
Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
Previous authors: JJ VERMUNT AND D M WEST
Current authors:
J J Vermunt - DVM, BAgSc, MSc, FANZCVS, Adjunct Professor in Dairy Cattle Health & Production, Veterinary Sciences, College of Public Health, Medical & Veterinary Sciences, James Cook University, Townsville, Qld 4811, Australia
MB Allworth - Professor of Livestock systems and Director of the Fred Morley Centre, School of Animal and Veterinary Sciences, Charles Sturt University, Wagga Wagga, NSW 2678, Australia.
Infectious diseases of the feet of cattle
Introduction
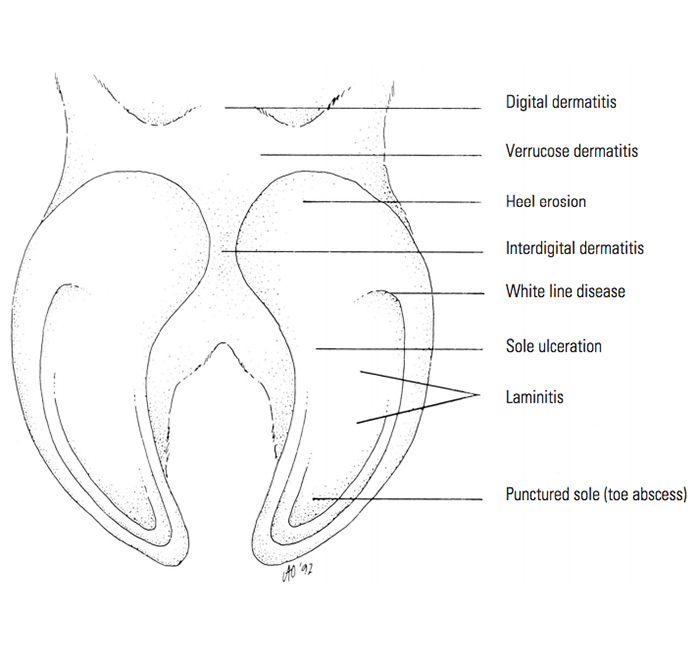
The lack of a standardized terminology is a serious limitation when studying the various infectious and non-infectious diseases of the feet of cattle.183 Different terms are often used to describe the same condition. In an effort to clarify the situation it has been decided that the name given to a particular disease should be based on the anatomical structures and the part of the feet involved (Figure 1) rather than on the aetiology, which is often of a multifactorial nature or in some conditions uncertain.183
Lameness in cattle is most commonly caused by conditions affecting the interdigital skin, or horn and corium (the latter being modified dermis) of the claws, whereas that which results from conditions affecting parts of the leg proximal to the feet (non-digital conditions) is relatively rare.129 The hind feet are affected by a greater variety of diseases and are also far more commonly involved than the front feet;7, 8 85 per cent of lesions involve the abaxial (or lateral) digits of the hind feet. In contrast, the prevalence of disease conditions in the medial and lateral digits of the front feet is more or less the same.
Infectious conditions— interdigital necrobacillosis (foot rot), interdigital dermatitis, bovine digital dermatitis and heel erosion — of the feet, of which interdigital necrobacillosis is the most important economically, account for approximately 70 per cent of cases of lameness.7, 8, 42 Interdigital necrobacillosis, interdigital dermatitis and to a lesser extent bovine digital dermatitis are common diseases worldwide which occur especially in dairy and beef cattle that are kept under intensive conditions, but they may also have a similar prevalence in cattle farmed under extensive conditions in areas with high rainfall and where muddy underfoot conditions prevail for prolonged periods.33, 107 Although interdigital necrobacillosis usually occurs as sporadic cases, 20 per cent or more of the animals in a herd may be affected over a period of several months.33 During wet conditions between 40 and 60 per cent of cattle are likely to be affected by interdigital dermatitis, but as it is typically a mild disease it is usually not diagnosed clinically and is therefore of little or no consequence.33
Collectively, the different conditions that affect the feet of cattle may cause significant economic losses. Studies have been done to determine the prevalence rates of some of them in affected herds in a number of countries.7, 8, 106, 169
In this chapter the infectious conditions of the feet of cattle (namely interdigital necrobacillosis, interdigital dermatitis and heel erosion) which are caused, or thought to be caused, primarily by Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus or Prevotella melaninogenica, (formerly Bacteroides melaninogenicus) are discussed, whereas the non-infectious conditions that affect the feet are only described briefly, and particularly with a view to distinguish them from some of the infectious conditions. Several groups of spirochaete bacteria of the genus Treponema are most likely involved in the aetiology of bovine digital dermatitis, as these organisms are consistently found in lesions of this infectious condition.95
Aetiology
The aetiologies of infectious conditions of the feet of cattle are multifactorial because of the interrelationships which exist between the infectious agents on the one hand, and the host and environmental factors on the other (see Epidemiology and Pathogenesis).
Several infectious agents, including F. necrophorum, D. nodosus, P. melaninogenica, and Trueperella (formerly Arcanobacter) pyogenes, as well as other facultative, spirochaetal and diphtheroid bacteria, have been isolated from cases of interdigital necrobacillosis and other diseases of the feet of cattle.15, 33
Of these bacteria, F. necrophorum is considered to be of primary importance in the aetiology of interdigital necrobacillosis, while the others, particularly P. melaninogenica, D. nodosus and T. pyogenes, may in some instances play a contributory role.15 Interdigital dermatitis is caused by benign strains of D. nodosus and is considered to predispose to interdigital necrobacillosis.33, 65, 93, 164, 168, 181, 183 The aetiology of digital dermatitis is not yet fully understood, but spirochaetes (probably Treponema spp.) have been regularly isolated from lesions. It is suggested that these invasive spirochaetes, with a predilection for keratinized cells, produce a toxin which is keratolytic.27, 130 Although the aetiology of heel erosion is not well defined, subclinical laminitis has been implicated in its aetiology.67, 68 Similarly, heel erosion can be a sequel to bovine digital dermatitis.95 It has also been suggested that there is an association between D. nodosus infection (interdigital dermatitis) and heel erosion.168 A recent study, however, has shown that D. nodosus was more common on healthy feet than on those with heel erosions.89 Other work suggests that heel erosion may be due to non-specific bacterial and chemical agents originating from faeces and urine.
Fusobacterium necrophorum is a normal inhabitant of the gastrointestinal tract of healthy herbivores and pigs, and is therefore commonly found in environments contaminated with faecal material. The pathogenic isolates of F. necrophorum that cause interdigital necrobacillosis belong to either biovar A or AB, and produce a soluble exotoxin, a leukocidin, as well as a haemolysin, while isolates that belong to biovar B produce little, if any, leukocidin or haemolysin, and are therefore less pathogenic.53
Most sheep, goats, cattle and farmed deer are carriers of benign strains of D. nodosus on their interdigital skin. In contrast to F. necrophorum, which can survive for several months in faecally contaminated, muddy conditions, D. nodosus does not survive in the external environment for more than two weeks under ideal conditions.153, 156, 179
For information on the general characteristics of F. necrophorum, D. nodosus and P. melaninogenica consult the introduction, Anaerobic, Gram-negative, irregular rods.
Epidemiology
One or more factors may play a role in the development of infectious diseases of the feet of cattle in a problem herd. These factors include the following:
- Certain anatomical features of the feet contribute to their susceptibility to infection. The relatively unprotected epidermis of the interdigital skin is frequently exposed not only to unhygienic, muddy conditions, which are the most important predisposing factor to interdigital necrobacillosis and interdigital dermatitis, but also to abrasions and trauma caused by a variety of objects, such as stones, cinders of walkways, stubble of harvested grain fields, plant awns and thorns, and tick bites. A favourable environment for the growth of bacteria and a portal for their entry into the underlying tissues are provided by changes in the integrity of the surface of the interdigital skin, if these are of a sufficient degree.81
- Infectious interdigital skin diseases, including interdigital necrobacillosis in cattle, often have a seasonal occurrence because wet environmental conditions predispose to them.81
- Bos indicus cattle breeds are generally more resistant to interdigital necrobacillosis than Bos taurus breeds.58, 107 A genetic predisposition to certain other conditions, such as interdigital hyperplasia, corkscrew claw, sole ulceration and laminitis, appears to be present in some lines of dairy breeds and this renders them more susceptible to these diseases.12, 181
- Zinc deficiency may predispose to interdigital dermatitis because of the production of a poorer-quality claw horn and interdigital skin. High concentrations of zinc are present in colostrum, with the result that a marginal zinc deficiency may occur in cows during early lactation. This deficiency can be exacerbated in cows that are fed a diet high in calcium during late pregnancy and early lactation. Even when the levels of zinc are adequate, excessive levels of calcium reduce the effective absorption and metabolism of zinc.
Other less important factors that predispose to interdigital necrobacillosis and other foot conditions in individual animals include conformational anomalies, which often only develop later on in an animal’s life, and result in increased mechanical stress on the claws,64, 167, 180 and metabolic stresses associated with pregnancy, parturition and lactation that result in softer, poorer-quality claw horn.9, 43, 144 Changes in the management and nutrition to which most cows are subjected to before or after calving may also play an important role in the occurrence of foot lesions.67 For example, the behavioural changes associated with the re-introduction of particular animals to the milking herd and the resumption of oestrus, together with possible changes in the housing conditions, may all increase the risk of injury to the animals’ feet.144

Pathogenesis
Fusobacterium necrophorum, D. nodosus, P. melaninogenica and T. pyogenes bacteria are incapable to invade intact skin. They can only penetrate when there is prior damage which, in the interdigital region, is usually in the form of maceration or mechanical trauma of the skin.
In infected tissues T. pyogenes produces a diffusible factor which stimulates F. necrophorum to multiply. It also consumes oxygen, resulting in a lowered redox potential in such tissues, thus enabling F. necrophorum, D. nodosus and P. melaninogenica to grow.15, 33 Fusobacterium necrophorum produces a leukocidin that is cytotoxic to phagocytic cells, thus protecting itself and T. pyogenes from phagocytosis. It also elaborates a dermonecrotic toxin and a vitamin K-like substance which is a growth factor required by P. melaninogenica. A collagenase that breaks down proteins to peptides and amino acids is produced by P. melaninogenica. The latter products contribute to tissue damage and are utilized by F. necrophorum during multiplication, but they in turn have a negative effect on collagenase production by P. melaninogenica.

Clinical signs and pathology
Interdigital necrobacillosis (foul-in-the-foot, interdigital phlegmon, bovine foot rot, phlegmona interdigitalis)
Interdigital necrobacillosis (Figure 2) usually affects only one foot, more commonly that of a hindlimb. Mild to severe lameness and, in the early stage of the disease, fever are common signs. Interdigital necrobacillosis is characterized by interdigital dermatitis and cellulitis of the interdigital area. The infection spreads rapidly into the soft tissues, causing a characteristic, symmetrical swelling of the tissues between the digits and around the heels, which in severe cases may extend to include the fetlock area.
Often there is also spreading of the claws and marked swelling and erythema of the coronary band, as well as the dorsal aspect of the interdigital area. As a result of the necrosis that occurs in the affected tissues, discharging sinus tracts which open to the externum in the skin of the interdigital region are sometimes present. Although pus is usually not present in large amounts, the necrotic lesion produces a characteristic odour. If the distal interphalangeal joint, whose capsule is in close proximity to the interdigital skin, becomes infected by extension of the lesion, septic arthritis may result, with consequent severe and prolonged lameness, rapid loss of weight and a marked drop in milk yield. Affected bulls may show temporary infertility. Septic tendovaginitis of the deep and superficial flexor tendons, culminating in their rupture, abscessation of the interdigital tissues and osteomyelitis of the digital bones may all be complications of interdigital necrobacillosis.33, 65, 125, 131, 180, 181
A condition called ‘superfoul’ or ‘super foot rot’, which causes severe lameness, was first described in the UK in the 1990s.34 It is a peracute form of interdigital necrobacillosis that produces severe interdigital necrosis with rapid extension deep into the surrounding structures, affecting the hindfeet or all four feet. The condition has suggested synergism with the causal agent(s) of bovine digital dermatitis and is refractory to conventional treatment. Septic arthritis is a common sequela if this type of severe interdigital necrobacillosis is not treated early and aggressively in its course.
Occasionally in early cases no external interdigital lesion may be visible, but there is severe lameness and swelling along the coronary band. Such cases are sometimes referred to as ‘blind fouls’ and usually respond well to parenteral antibiotic treatment.
Interdigital dermatitis (stable foot rot, scald, dermatitis interdigitalis)
Interdigital dermatitis is a poorly described condition of the superficial surface of the epidermis of the interdigital skin and occurs commonly in cattle that are housed for long periods, usually under unsanitary conditions. It is characterized by erosion and hyperkeratosis (Figures 3a and 3b), usually without fissure formation or extension of the inflammatory process into the deeper tissues of the feet.33, 65, 125 A somewhat foul odour may be present and the lesion is painful to the touch. More than one foot is commonly affected. The lesions are usually most obvious at the bulb of the heels and result in slight swelling of the adjacent soft tissues. This may be followed by separation of the horn on the inner aspects of the heels, which facilitates the entry of foreign material between the horn and the underlying corium, resulting in a proliferative inflammatory reaction. In most uncomplicated cases there is usually no evidence of lameness, although some animals may be mildly lame and paddle.
The causative agent has not been conclusively established, but D. nodosus may be isolated. Experimental infection of cattle with D. nodosus can produce a lesion that is similar to scald in sheep, which is also known as interdigital dermatitis. However, it has now become increasingly clear that most cases of interdigital dermatitis in cattle are in fact bovine digital dermatitis of the interdigital space. In Europe it can be a common presentation of the disease and may be more likely to cause lameness than typical bovine digital dermatitis.

Heel erosion (slurry heel, chronic necrotic pododermatitis, erosio ungulae)
Heel erosion is characterized by the development of lines of erosion varying from small black, pitted marks, circular craters to deep cracks or terraces on the plantar/palmar convexity of the bulb of the heels.65 (Figures 4a and 4b). As the condition progresses, the lines of erosions form V-shaped clefts with the apex of the ‘V’ pointing dorsally and the clefts penetrating deeply towards the corium.65 Heel erosion is relatively insignificant as a direct cause of lameness. However, because of the gradual loss of horn from the bulb surface of the heels, it leads to a reduced shock-absorption capacity of the digital cushions and a consequent reduction in their ability to transfer concussion to the sole, thus predisposing to other claw conditions (white line disease, insufficient wear of the wall of the claw, sole ulcer, heel ulcer, sole abscess).65 Heel erosion is often followed by overgrowth of poor-quality horn directly anterior to the erosion. This wedge of abnormal horn causes pressure on the sensitive corium, which becomes inflamed and painful.95
Heel erosion is a common finding in housed dairy cows during the late winter months, but the exact aetiology is still much debated. Although bacteria such as D. nodosus have been regularly linked to heel erosion, it has become clear that it can also be a sequel to bovine digital dermatitis, so it is often treated as an infectious disease.



Bovine digital dermatitis (papillomatous digital dermatitis, strawberry footrot, hairy foot warts, heel warts, Mortellaro disease, dermatitis digitalis)
Bovine digital dermatitis is a painful condition characterized by dermatitis followed by erosion and superficial ulceration of the skin bordering the coronary band above the heels (Figures 5a and 5b). The lesion has a white border and a surrounding area of proliferative dermatitis.181 Worldwide, this disease has become the most important infectious cause of lameness, especially in dairy cattle; the condition appears to be uncommon in beef cows and growing cattle. Recently, however, bovine digital dermatitis has been identified as an emerging issue in beef cattle in the UK.157 In housed cattle it can cause substantial economic losses and require considerable effort to effectively manage.95 Prevalence figures from 2 per cent to 25 per cent are reported in affected dairy herds, with outbreaks common after the introduction of purchased cattle.145 In addition, the bacteria associated with bovine digital dermatitis have been detected in a range of ‘non-healing’ bovine claw disorders, including white line disease and sole ulcer.54
Even though several aspects of the aetiology and pathogenesis of the disease have been identified, the causal agent is still under debate. Although it is widely accepted to be spirochaete infection the role of Treponema spp. in the development of lesions is still to be clarified. The condition is linked to prolonged exposure to slurry and wet underfoot conditions; however this fact alone does not explain the low prevalence in housed beef herds. Lesions are commonly found on both hind feet; they are much rarer on the front feet.
The most common presentation of bovine digital dermatitis is as a painful inflammation of the skin immediately above the coronary band between the heel bulbs. Clinically, bovine digital dermatitis presents as a dynamic process with morphologically distinct stages. A variety of classification systems used to describe the stages of bovine digital dermatitis development have been described, with the most widely adopted being the M‐stage scoring system.20 This system identifies five categories where M0 is defined as normal digital skin with no evidence of dermatitis; M1 if a small (<2 cm in diameter) circumscribed red to grey epithelial defect is present; M2 if an ulcerative active ≥2 cm in diameter with a red‐grey surface; M3 (healing stage) after M2 lesion surface becomes firm and scar‐like; M4 (chronic stage) if the lesion surface is raised with brown or black tissue, hyperkeratotic, scaly or proliferative; and M4.1 defined as small red circumscribed lesions occurring within the boundaries of an existing M4 lesion. Lesions of the early, acute stage can have a characteristic foul smell, are painful upon palpation and prone to bleeding after their surfaces are touched.
Bovine digital dermatitis lesions can also occur in the dorsal aspect of the interdigital space and along the coronary band, away from the heel bulbs.95 There is usually no swelling of associated tissues, irrespective of where the lesion is situated. A common finding, especially in relatively small lesions, is heel erosion; as the lesions persist, the erosions spread and can progress to under-running of the horn of the sole.
Diagnosis and differential diagnosis
As lameness in cattle is most commonly caused by disease of the feet, their careful examination, after they have been thoroughly cleaned and trimmed, is of the utmost importance in order to establish an accurate diagnosis. Conditions responsible for lameness in cattle may, for the sake of convenience, be divided into:
- those that involve the interdigital skin,
- those that affect the horn and corium of the claws, and
- those that affect the tissues of the limbs proximal to the feet.
Conditions that affect the interdigital skin or the horn and corium of the claws (Table 1) may be collectively termed digital diseases.7 Readers should consult other sources70, 77 for information on the conditions that affect the tissues proximal to the feet.
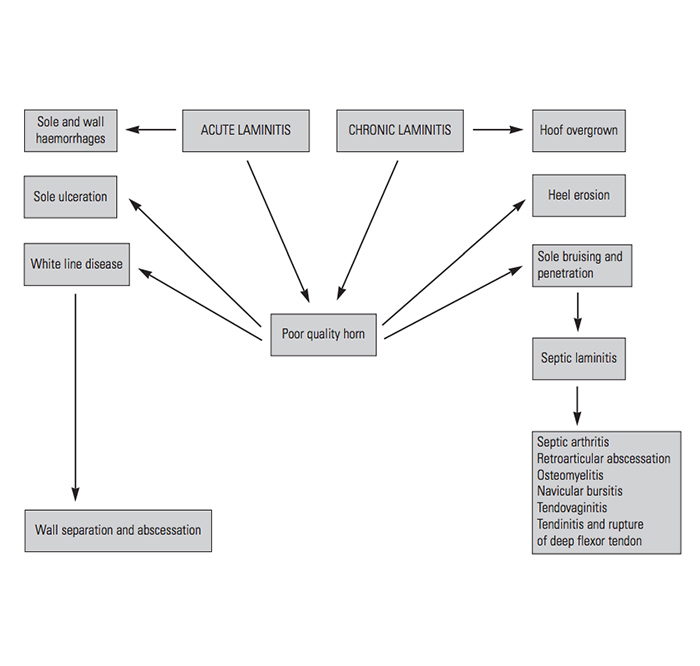
The location of some of the common conditions that affect the feet are illustrated in Figure 1 and listed in Table 1. Of these sole ulcer, punctured sole (sole abscess), white line disease, laminitis and heel erosion are inextricably intermingled — the production of poor-quality horn being a common factor (Figure 7).182
Table 1 Classification of some diseases of the interdigital skin, or the horn and corium of the claws of cattle. (Adapted from Weaver182)
| SKIN | HORN AND CORIUM |
|---|---|
| Interdigital necrobacillosis (foot rot) | Sole ulcer |
| Interdigital dermatitis | Punctured sole (sole abscess) |
| Interdigital hyperplasia | White line disease |
| Verrucose dermatitis | Laminitis |
| Bovine digital dermatitis | Heel erosion |
Although any condition that results in lameness could probably be confused with interdigital necrobacillosis (foot rot), retro-articular abscess, interdigital foreign body, septic arthritis of the distal interphalangeal joint, septic sand crack, white line disease and interdigital dermatitis are most commonly confused clinically with it.65 The swelling that is associated with retro-articular abscess is not symmetrical and is restricted to the heel of only one digit; this being in contrast to interdigital necrobacillosis, in which there is symmetrical swelling of the affected region of both digits. Septic arthritis of the distal interphalangeal joint can be distinguished from interdigital necrobacillosis in that the oedematous swelling is proximal to the coronary band, and that it affects only one digit and is first noticed on the dorsal aspect of the digit. A distinguishing characteristic of a septic sand crack is that the inflammatory oedema proximal to the coronary band is localized to the dorso-abaxial quarter of the digit. In white line disease the oedema is proximal to the coronary band and is usually confined to the area just dorsal to the heel. Interdigital dermatitis is sometimes confused with interdigital necrobacillosis, but it produces only mild, if any swelling of the feet, no systemic signs, and usually no (or only mild) lameness, all of which are usually pronounced features of severe interdigital necrobacillosis.
Verrucose dermatitis (heel warts, dermatitis verrucosa)
Verrucose dermatitis is a chronic, moist, proliferative wart-like inflammation of the plantar or palmar skin above the heels of the hind claws characterized by a mass of filiform fronds. Affected animals show slight lameness as a result of the mass of abnormal tissue.125, 181 The occurrence of verrucose dermatitis is generally sporadic, but occasionally a number of cases may be present simultaneously in a herd. While the precise aetiology remains undetermined, factors that cause chronic irritation could play a causative role.125, 181
A typical lesion is a circumscribed, moist ulcerative erosive area that is painful to the touch. The raw‐red granular appearance of the lesion resulted in one of its alternative names, being strawberry foot rot, although the disease is also known as hairy footwart, hairy heel warts, raspberry heel, Mortellaro's disease, papillomatous digital dermatitis and verrucose dermatitis. Notwithstanding, bovine digital dermatitis is likely the most accurate and commonly used term, and it is now widely accepted that verrucose dermatitis denotes the acute, granulomatous (M2) stage of bovine digital dermatitis.120
Interdigital skin hyperplasia (interdigital fibroma/granuloma, interdigital warts, corns, keloids, limax, hyperplasia interdigitalis)
This condition refers to excess epidermal and hypodermal tissue occupying part or all of the interdigital space. It is a chronic, hyperplastic inflammation of the interdigital skin that commonly affects both hind feet. The condition usually appears as a protuberance of skin at the front of the interdigital space (Figure 8). It normally does not cause lameness unless the mass of hyperplastic tissue is abraded as a result of necrosis caused by pressure against the axial side of the horny walls of the claw, or if it becomes infected. The degree of lameness usually depends on the severity of hyperplasia and superimposed bacterial infections. 125, 180, 181
If interdigital hyperplasia occurs in both hind limbs in animals less than two years old it is probably precipitated by an inherited anatomical defect, such as an abnormally wide interdigital space and abaxial angulation of the middle and distal phalanges,181 with some breeds (Herefords) being over-represented. Chronic mechanical irritation and infectious agents may also play a role in inducing or exacerbating the condition.
Laminitis (founder, aseptic pododermatitis, pododermatitis aseptica diffusa)
Laminitis is a commonly used but often poorly understood term. Its technical definition is aseptic pododermatitis, or inflammation of the dermis of the laminar region of the extremities of ungulates. As such, it is a pathological diagnosis not a disease, although laminitis is often used to stand for more than just pathology. In cattle, laminitis is often used to mean anything that starts the process of claw horn damage, especially where there is a suspected nutritional component. Nowadays three types of laminitis are recognised: acute, chronic and subclinical.95
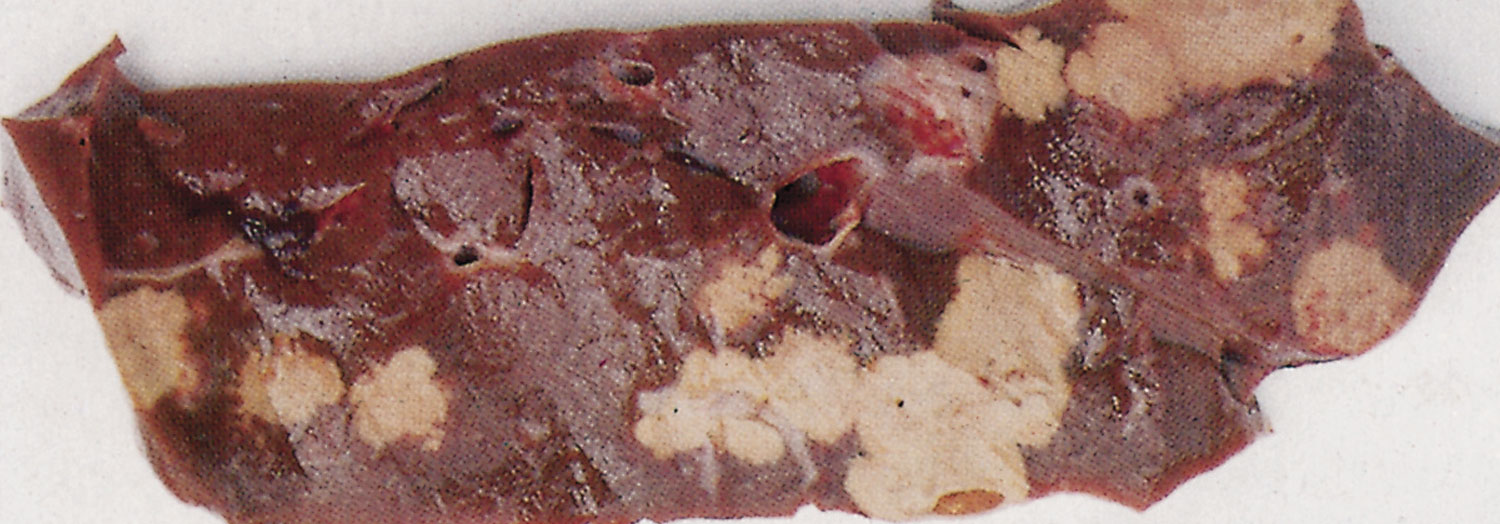
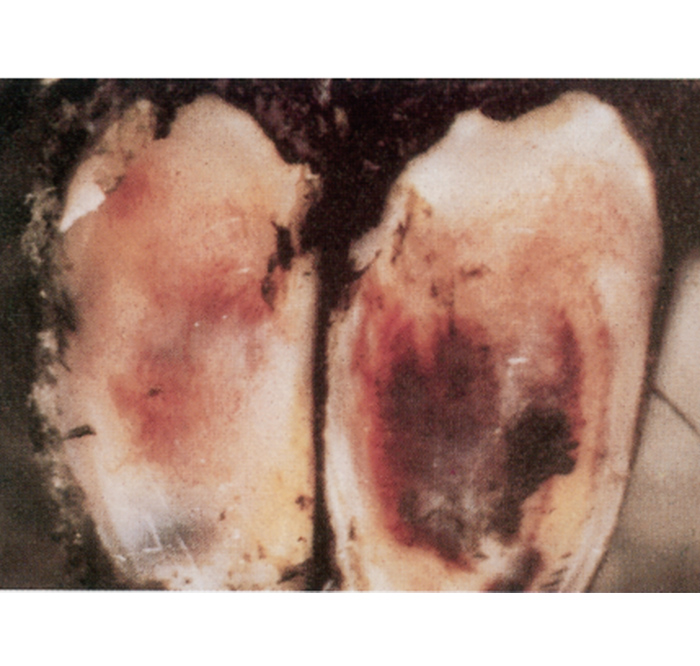
Acute laminitis is an aseptic inflammation of the corium (dermis) which coincides with a systemically sick animal. It is not a common condition in cattle, but may follow grain overload (acute rumen acidosis) or some other acute illness. It has a rapid onset and presents as pain with various degrees and types of lameness, resulting in aberrations in stance and gait. As in the equine species, affected cattle may take on a characteristic stance with both fore- and hindlimbs extended forward. Nonetheless, there can be significant variation in the aberration of gait, and sometimes only one foot may be involved. Affected animals tend to walk stiffly and with an arched back. The condition is characterized by warm and painful claws, severe lameness, stiffness, elevated body temperature, increased heart and respiratory rates, and loss of appetite.119 Only one, or more claws may be affected, but more commonly all four feet are involved. Sole and wall haemorrhages are not a feature of acute laminitis, but are characteristic of subclinical laminitis (Figure 6). Such haemorrhages should not be confused with severe bruising (Figure 9).
Subacute laminitis is a mild form of acute laminitis. Both forms of laminitis may be a transient state, but they consistently progress to variable degrees of chronic laminitis.
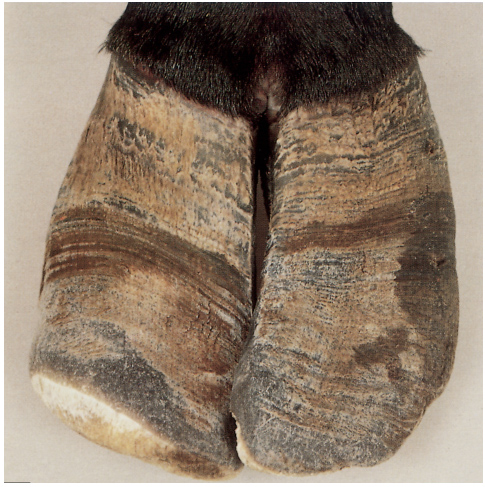
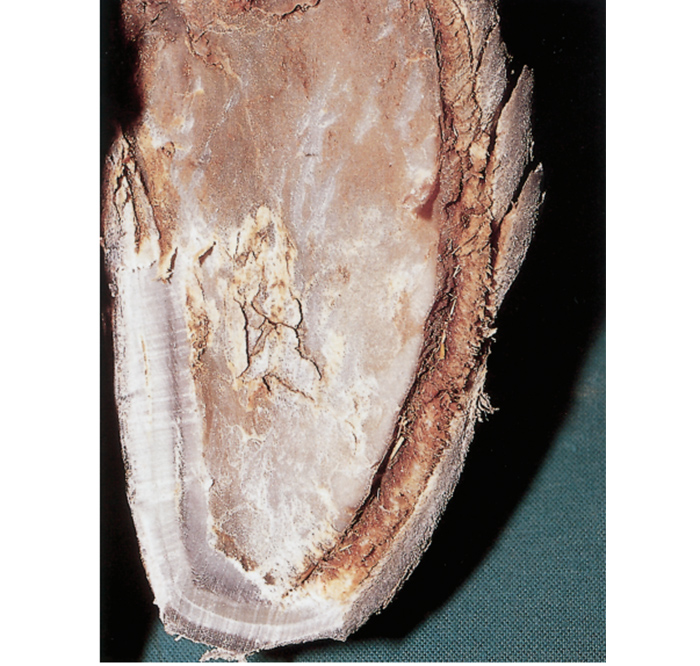
Chronic laminitis has no generalized systemic signs, but lameness and stiffness are present. This condition develops over a prolonged period of time; successive episodes of laminitis (which may not all be clinical) lead to the dorsal claw wall becoming concave and irregular grooves and ridges in the dorsal claw wall, which diverge towards the bulb, being present in the claw wall (Figure 10). There is often a yellow or red discoloration of the horn of the flattened and broadened sole. Sole ulcers and a widened white line are also common features (Figure 11). Because of the production of poor-quality horn, laminitis is a major predisposing factor for many of the other conditions of the claws (Figure 7).31, 67, 68, 182
In contrast to acute and subacute laminitis, subclinical laminitis is not defined by easily observable clinical signs. Generally, subclinical laminitis is diagnosed based on observed changes in the claw horn; i.e. deteriorated horn quality (soft, yellowish and waxy) and haemorrhages in the weight-bearing surface of the claw (especially the white line, apex of the sole and axial side of the sole-heel bulb junction) or in the abaxial claw wall. These haemorrhages are distributed over all claws in a fairly symmetrical manner.
Laminitis is a poor term to use for these changes even if the strict technical definition is used, because the principal pathology driving the changes is degeneration of the dermis or corium (i.e. a coriosis, not a laminitis). However, the fundamental problem with defining these changes in the claw horn as being ‘subclinical laminitis’ presumes a process, when all there is an outcome.
The commonly accepted hypothesis linking nutrition and subclinical laminitis has been that toxic substances, such as histamine, lactic acid, serotonin and endotoxin, are formed or released in the digestive tract (mainly as a consequence of subacute rumen acidosis). These substances are also thought to be produced during postpartum diseases. These toxic, vasoactive components, together with a coagulopathy, are believed to severely disrupt the micro-vasculature and haemodynamics of the corium, leading to tissue hypoxia and nutrient starvation, followed by ischaemic necrosis and degeneration of the horn-producing structures. Furthermore, an inadequate supply of sulphur-containing amino acids reaching the keratin-producing cells could lead to lower levels of disulphide bonding in the keratin tissue and, consequently, synthesis of structurally incompetent horn or cessation of keratinisation.68, 70 The disulphide bonding in keratin gives the claw its structural integrity. In all, these changes result in permanent damage of the claw. Nevertheless, almost 40 years after the development of the concept of subclinical laminitis and its association with a nutritional insult this process remains an unproven hypothesis.
More recently, a series of innovative studies at the University of Bristol clearly showed that the changes in claw horn associated with subclinical laminitis could be produced by parturition.90, 160 As part of the process of parturition, triggered by the action of matrix metalloproteinases, there is weakening of the suspensory apparatus that secures the distal phalanx within the claw horn capsule. The distal phalanx becomes more mobile and can ‘sink’ within the claw. These changes can then lead to compression and damage of the corium (both of the white line and sole) situated beneath the distal phalanx. This damage produces haemorrhages (Figure 6) and affects the integrity of the claw horn produced, thereby increasing the risk of claw horn diseases, such as sole ulcer, double soles and white line disease.
The parturition-related changes are relatively short-lasting (up to 12 weeks after calving), but may have long-term and substantial impacts when they combine with other stressors, especially environmental factors, such as spending long periods standing on concrete. Poor nutrition management, particularly if it leads to subacute rumen acidosis, is another potential stressor, although it is unlikely to be the most important.95
One critical factor which can influence the impact of the parturition-associated changes is the protection that is provided by the digital cushion. This structure consists of three parallel pads of fat that run longitudinally from the heel to underneath the distal phalanx; their function is to disperse the shock associated with the foot landing on the ground. Thus, if the digital cushion is thin, then it is likely to provide less protection to the corium, resulting in increased risk of damage to the corium. It has been reported that the prevalence of claw horn disease was significantly associated with thickness of the digital cushion, with thinner digital cushions being associated with increased risk of diseases.23, 117 In addition, a follow-up study showed that thin digital cushions were also associated with increased claw horn haemorrhages.118 Three reasons have been put forward for the digital cushion being thin, other than the mobilisation of body fat: (i) differences in digital cushion development in early life, (ii) previous lameness, which could cause damage and changes to the digital cushion, or (iii) laxity in the suspensory apparatus, as occurs around parturition,118
The relative proportions of individual fatty acids in the digital cushion are different from those in the rest in the animal’s adipose tissue. This difference may be related to the shock dissipating function of the fat in the digital cushion; thus changes in fatty acid composition of the cushion may influence its protective effect.127 Further research is required to better understand such changes, in particular the influence of nutrition, age and previous lameness history on the composition of the digital cushion and the protection it provides.


Sole ulcer (ulceration of the sole, Rusterholz ulcer, pododermatitis circumscripta)
Sole ulcer is circumscribed loss of the sole horn, exposing the corium (dermis) of the sole. Sole ulcers are typically located in the region of the sole-heel bulb junction, usually nearer the axial margin of the claw (Figure 12). Bilateral involvement of the lateral digit of the hind feet is common, especially in high-yielding dairy cattle (commonly Holstein-Friesians) that are kept on concrete, although the lesion is often more advanced in one of the claws. Lameness is usually not severe unless granulation tissue is formed which extends from the corium and prolapses through the defect in the sole.125 Sepsis may complicate sole ulceration and result in septic laminitis, osteomyelitis, septic arthritis of the distal interphalangeal joint, necrosis and rupture of the deep flexor tendon, and abscessation.
The site of a sole ulcer is specific, namely immediately distal to the axial prominence and plantar process of the distal phalanx (flexor tuberosity). Most authors agree that sole ulcer is caused by local damage, such as compression of the corium accompanied by haemorrhage. The function of the horn-producing cells in this area is compromised and faulty horn, or horn of poor quality, is formed, or a complete shutdown of horn production occurs. As such, laminitis may predispose to this condition (Figure 7).125, 182
Heel ulcer (sole fracture, necrotic heel tract)
In most surveys heel ulcers are less commonly reported than sole ulcers. The lesion occurs in the centre of the sole, at the junction between the harder sole horn and the softer heel horn (i.e. a little further caudally than the typical location of a sole ulcer). The precise cause of heel ulcers is unclear, but it has been proposed that the lesion may be caused by pinching of the corium under the caudal edge of the distal phalanx.26 The abaxial border of the posterior edge of the distal phalanx is situated more caudal and occupies the central sole area, whereas the flexor tuberosity of the distal phalanx is anterior and axial to this site. This could explain the similar pathogeneses, but different sites, of heel ulcer and sole ulcer lesions.95
Toe ulcer (toe abscess, white line disease at the toe)
Toe ulcers are believed to be the result of excessive pressure from the cranial margin of the distal phalanx. In many cases, the white line in the toe region may only be stained with blood or serum. In more advanced cases, penetration of the sole may take place, with associated infection. Severe, complicated lesions may result in separation of the sole and osteitis of the tip of the distal phalanx.95
The incidence is usually sporadic, but outbreaks may occur. For example, toe ulcers and vertical fissures (sand cracks) are the most common causes of lameness in bulls held at AI centres in New Zealand.174 One explanation could be that the intense haemorrhage in the toe area of the front claws is caused by trauma when bulls are dismounting. The condition is also linked to thin soles (excessive wear), which may be caused by either zealous over-trimming of the sole or concrete walking surfaces. Toe ulcers are also reported to be a common condition in pasture-grazed dairy cattle in South America (Uruguay, Argentina and Chile).
White line disease (white line abscess, lesion or injury)
In general, the term ‘white line disease’ refers to the conditions of haemorrhage, fissure and abscess formation that most commonly occurs in the abaxial white line of the lateral hind claw, two-thirds of the way back from the toe, immediately distal to the bulb of the heel.95 In heifers at pasture, white line disease is more commonly seen at the abaxial wall of the medial front claws.30
The white line or ‘white zone’ is the cement junction between the wall of the claw and the sole and, as such, is a point of weakness.70 One particular type of horn merges into another, at which point the horn is softer than elsewhere and disintegration occurs easily. Inflammation of the laminae and corium may further weaken the white line. Separation, followed by impaction, penetration of the corium, infection and abscessation of the white line are the commonly recognized clinical lesions. Once separation occurs, small fragments of dirt or even stones may be forced into the defect (Figure 11). Following entry and multiplication of bacteria the resulting infection forms an abscess. The infection usually tracks proximally and caudally along the direction of the dermal lamellae of the wall (septic laminitis), rather than beneath the sole, and often leads to a discharging abscess and/or sinus formation at the coronary band. Alternatively, the infection may track inwards and involve the deeper tissues of the claw, resulting in deep digital sepsis (e.g. retro-bulbar abscess and septic arthritis of the distal interphalangeal joint). Likewise, heel abscesses may occur as a consequence of white line disease. White line abscesses occurring towards the toe are more likely to under-run the entire sole, rather than track proximally up the lamellae to discharge at the coronary band.
Most lesions are observed in the region of the abaxial border of the sole just cranial to the heel bulb. The toe area is the next most common site. In the hindlimb, the abaxial border of the claw is the area of maximal impact forces during locomotion and absorbs the highest pressures during mid-stance. It is also subjected to torsional forces as the cow turns sharply. In the forelimb, the abaxial border of the sole near the toe receives the greatest concussion on impact.
Predisposing factors in the aetiology of white line lesions are excessive walking on hard surfaces, excess twisting and turning of cows whilst in the milking yard, wet and dirty underfoot conditions that soften horn, claw deformities (in particular overgrowth of the toe) and other factors which produce corium damage. Damage to the corium of the white line leads to haemorrhages in the white line, which, combined with a decline in horn quality (as a direct result of the corium damage), reduces the strength and integrity of the white line.
Punctured and under-run sole (sole abscess, sole penetration, septic traumatic pododermatitis, pododermatitis septica)
Punctured and under-run sole is a common condition of the claws, being a diffuse or localized septic inflammation of the corium (pododerma) of the sole. The condition often has a traumatic origin involving nails, sharp stones or excessive abrasion. If the horny capsule is penetrated dirt and bacteria accompanying such penetration cause a purulent and/or necrotic infection of the underlying soft tissue (mainly corium).131 A similar infection may occur through very small defects (e.g. small cracks) in the white line or other areas of the sole. Animals with soft horn will obviously be predisposed.
Sole penetrations can occur in normal claws (e.g. as a result of a nail or other sharp object), but are seen more commonly in claws that have been worn thin. In such cases, a sharp stone may readily penetrate the thin layer of sole horn, with poorly maintained cow tracks being a major problem in grazing herds.95
Vertical fissure or ‘sandcrack’
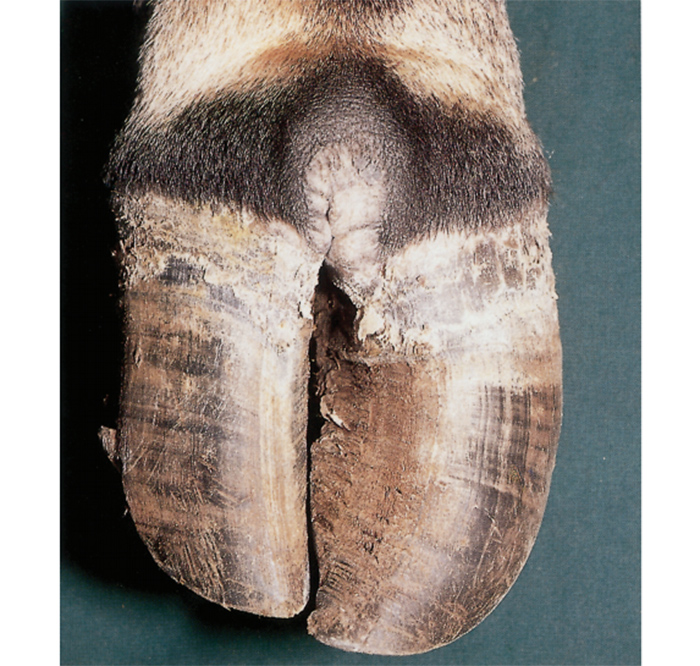
Vertical fussures occur on the dorsal or dorso-abaxial side of the claw wall, especially on the forelimbs (Figure 13). There is a loss of continuity of horn fibres of the dorsal claw wall extending for a variable distance from the coronary band toward the bottom of the claw wall. Fissures that extend through the full thickness of the horn down to the underlying lamellae cause considerable lameness, but usually not otherwise. Those that involve the coronary band and become secondarily infected are serious and may result in infection of the dorsal pouch of the distal interphalangeal joint capsule. A vertical fissure may develop when claw horn becomes dehydrated and splits, such as when the periople, which restricts evaporation of water from the wall, is damaged by excessively dry, warm and windy conditions.66, 70, 125 Sandy soils and trauma to the coronary band are further predisposing factors. Deficiencies of the trace minerals zinc and copper have also been implicated in the aetiology of vertical fissures.189
Horizontal fissure or ‘thimble’
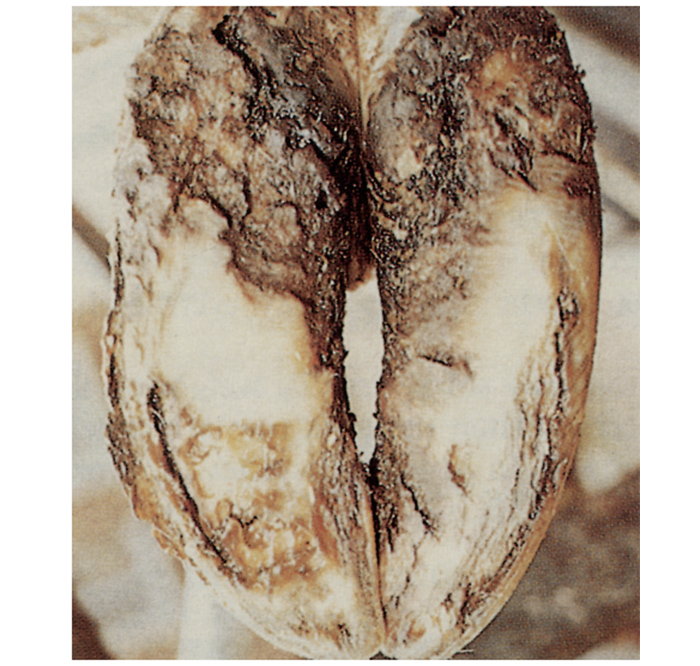
A horizontal fissures presents as a discontinuity of the claw wall, running parallel to the coronary band. It occurs sporadically and is due to a temporary, but complete interruption of horn production. The disorder is generally related to a severe upset in metabolism, such as acute laminitis, severe endotoxaemia or systemic illness (e.g. an acute febrile disease, such as coliform mastitis or metritis around the time of calving), acute rumen acidosis, severe facial eczema or malnutrition (starvation).66, 125 Several months after such an event, a groove is evident in the horn running parallel to the coronary band. As the horn grows (at approximately 5 mm per month), the defect may separate from the healthy horn proximally (Figure 14), usually when it reaches halfway down the distance from the coronary band to the toe. The corium remains intact distal to the horizontal fracture holding the distal claw horn attached at the toe. Such a fissure will move when weight is taken, tensing the underlying laminae and causing variable lameness.145 Occasionally debris can become impacted in the fissure, causing abscessation. Horizontal fissures may occur in one or more claws of the same animal. Occasional cows may have all eight claws affected, or at least have evidence of interruption in horn growth on all claws.
Management
Because this chapter mainly focuses on F. necrophorum, D. nodosus and Bacteroides spp. infections, the emphasis in this section will be on the management thereof.
The main methods used in the control of interdigital necrobacillosis (foot rot) are the elimination or reduction of the exposure of the feet of cattle to the major risk factors (wet, muddy, unhygienic conditions and trauma caused by stony patches in laneways and yards), the use of prophylactic foot-bathing, and the prompt application of chemotherapy (usually parenteral antibiotics; rarely topical treatment nowadays). Vaccination to prevent foot rot has been applied, but with variable success.Vaccines against F. necrophorum are available in the US, but their principal use is against the development of liver abscesses, with foot rot prevention a very much secondary consideration.
Adequate restraint of an affected animal is necessary in order to allow proper examination of the claws and to apply effective local treatment. This can be achieved by the use of mechanical leg lifters, mobile crushes or tilt tables, by casting the animal on the ground, or lifting the affected leg by means of a rope using one of several well-tried methods.70, 95, 125, 131 Chemical restraint can also be used to quieten an animal, particularly during examinations of the hind legs; in most animals a small dose of xylazine (10 to 20 mg) given intravenously will make it possible to lift a hind leg with or without the use of ropes. This form of restraint, however, is not suitable for examining a front foot, as the animal tends to lie down when a front foot is lifted.
In animals suffering from a very painful digital condition, regional anaesthesia by interdigital nerve block or intravenous regional anaesthesia may have to be resorted to in order to carry out an adequate examination and application of local treatment. Both techniques are quick and simple. However, it should be realized that an interdigital nerve block anaesthetizes only the axial aspects of the digits; hence, it is not suitable for treating lesions that are located abaxially. It is performed by injecting 20 ml of a suitable local anaesthetic solution between the digits 20 to 30 mm distal to the fetlock while the animal is in a standing position and lightly sedated, at the same time restraining it by lifting its tail and pushing the latter forward.
When using intravenous regional anaesthesia any accessible and prominent superficial vein situated distal to a previously applied tourniquet may be chosen. The most common site for the hindlimb is the lateral branch of the saphenous vein, and for the forelimb the medial branch of the cephalic vein. Alternatively, it may be easier to use the dorsal common digital vein III, or to tap into any venous plexus on the dorsal or plantar/palmar aspect of the limb, exactly in the midline and 2 to 3 cm below the fetlock joint (i.e. at the level of the proximal interdigital joint).95
A strong rubber tourniquet is placed around the limb just below the tarsal/carpal region and the vein palpated immediately proximal to the fetlock joint. The area over the vein is disinfected and 10 to 20 ml of a 2 per cent lignocaine solution (without adrenaline) is injected intravenously using a 20 gauge needle. Analgesia starts to develop after two to three minutes and is complete within 10 minutes. The interdigital region is the last area to become fully numb and increased amounts of anaesthetic solution (up to 30 ml) may be required to achieve adequate analgesia.95 After releasing the tourniquet, sensation and motor function return to normal in about five minutes.
Once adequate restraint of the animal has been achieved, the affected foot is thoroughly cleaned. The affected interdigital skin, heel horn and surrounding soft tissue, including the coronary band, are carefully examined to assess the depth of penetration of the infection, and the presence of cellulitis and heel horn erosion. The existence of discharging sinuses which usually occur in neglected or advanced cases of other lameness-causing conditions indicates that the infection has spread to the deeper structures of the digit. Swelling at the coronary band or in the interdigital area may indicate a build-up of pus under the sole. Hoof testers may be used to assist in the location of painful areas in the sole, but if xylazine was used as a means of restraint, or if regional anaesthesia was applied, the response of the animal to hoof testers will be inconclusive. Sloughed and necrotic interdigital tissue and heel and sole horn should be removed using a hoof knife. During this procedure special attention should be given to the axial region to ensure that the interdigital space is sufficiently exposed to prevent dirt and dung from being trapped.


Table 2 Some therapeutic agents used for the topical treatment of interdigital necrobacillosis and other interdigital infectious diseases in cattle
| AGENT | METHOD OF USE |
|---|---|
| Antibiotic and antimicrobial mixtures. Commonly contain sulphanilamide, sulphadiazine, oxytetracycline Metacresolsulphonic acid | Apply as an ointment, a powder or an aerosol Daily topical application of concentrate |
| Hydrogen peroxide | Daily topical application of concentrate |
| Acriflavine:glycerine mixture | Commonly used under a bandage (as a 1:100 concentration) |
| Glycerine ichthamol BPC | Commonly used under a bandage |
| Povidone iodine | Apply as an ointment or a spray |
| Gentian violet | Apply as a spray in combination with antimicrobial mixtures |
Following the removal of all necrotic and under-run horn, any cracks should be trimmed and cleaned out and excessive granulation tissue removed. If the heel bulb is overgrown, the excess heel horn should be pared away. If necessary, the toe should be shortened such that the vertical weight-bearing axis is moved forward.
Interdigital dermatitis does not respond satisfactorily to the standard treatments used for interdigital necrobacillosis, but local treatments are usually effective. The type of topical therapy to be applied will depend on the nature and severity of the infectious condition. In cases of interdigital dermatitis, topical dressing with a 1:1 mixture of anhydrous copper sulphate and sulphamethazine (sulphadimidine) usually results in rapid healing.65 Footbaths containing a 5 to 10 per cent solution of formalin or copper sulphate may be used to further control the condition. Good results have also been obtained if it is used as a 5 per cent solution on alternate days for two weeks. A mixture of 10 per cent copper sulphate in slaked lime (calcium hydroxide) is often used in the same manner.
Various therapeutic agents used in the topical treatment of interdigital necrobacillosis and other infectious diseases of the feet are listed in Table 2
In cases of infectious interdigital conditions bandaging of the affected foot is normally not required, but it may be considered if the housing conditions are very unhygienic or the lesions are extensive. In such cases, the interdigital area should be bandaged loosely to assist drainage. Medicated gauze, cotton wool padding and adhesive bandage are used. The bandage should be removed after three to five days and replaced only if deemed necessary.
Bandaging between the claws, as part of managing interdigital lesions, is generally contra-indicated because this practice separates the claws and tends to open any lesions.95 Also, bandages absorb moisture which may carry infection towards the lesion. Wiring the toes together, or strapping the claws together using an elastic adhesive bandage or strong plastic tape, aids healing of interdigital wounds.
Systemic antimicrobials should be administered in cases of infectious digital disease where there are signs of deep penetration of the infection, as is often the case with interdigital necrobacillosis. A list of the common antimicrobial agents used in the therapy of infectious disease of the feet is given in Table 3.
Table 3 Antibiotics and antimicrobial drugs used for the systemic treatment of infectious digital diseases in cattle
| ANTIBIOTIC/ANTIMICROBIAL | DOSAGE AND ROUTE |
|---|---|
| Procaine penicillin G | 20 000 – 30 000 IU/kg BW im once or twice daily for 3 days |
| Ampicillin trihydrate | 5 – 10 mg/kg BW sc or im once a day for three days |
| Oxytetracycline | 10 mg/kg BW im or iv once a day |
| Sulphamethazine 33% solution | 0,2 gm/kg BW initial dose followed by 0,1 gm/kg iv once a day |
| Sulphadimethoxine | 1 ml/10 kg BW im once a day |
| Sulphonamide-trimethoprim combination | 15 – 24 mg/kg BW im or iv once a day |
| Tylosine | 10 mg/kg im BW once a day |
| Ceftiofur | 1 – 2 mg/kg BW once a day for 3 days |
| Sodium sulphadimidine solution | 150 – 200 mg/kg BW iv |
| Florfenicol | 20 mg/kg BW im, repeated after 2 days, or 40mg/kg sc given once |
im = intramuscularly
iv = intravenously
sc = subcutaneously
BW = body weight
The use of non-steroidal anti-inflammatory drugs, such as flunixin meglumine, ketoprofen and meloxicam, is recommended for animals in pain.
Immediate remedial action is required for cases of ‘superfoul’.145 Under intravenous regional anaesthesia, the interdigital lesion should be debrided and packed with clindamycin tablets. A bandage should then be applied. The animal should be given systemic antibiotic (e.g. tylosine) and non-steroidal anti-inflammatory therapy (e.g. flunixin), and isolated in a well-bedded straw pen.
When complications such as septic joint disease, sole ulceration or suppurative tendosynovitis occur, a support block (or similar) may be attached to the sound claw in order to lift the affected claw off the ground. The block should be shaped to that of the normal claw and fixed to it with an adhesive compound. Care must be taken that the normal weight-bearing mechanism of the sound claw is not disturbed after the block has been fixed in position. Other procedures such as provision of adequate drainage or induction of ankylosis of an infected joint should also be considered. If there is deep infection, the affected claw should be amputated. In this case, both claws of the other hindlimb must always be carefully examined first to ensure they are sound.
The best way to control infectious digital disease is by eliminating or restricting exposure to predisposing factors such as faecally contaminated, muddy conditions. Poor claw care (lack of or unsatisfactory preventive claw trimming) increases the exposure of the interdigital skin to trauma and wet conditions. Where practical, claws should be trimmed twice a year. 64
Foot-bathing can be used to prevent infectious interdigital conditions of the feet. It not only cleans the claws and interdigital skin, but also inhibits the growth of bacteria and hardens the interdigital skin. Two footbaths should be used, one containing only water to wash the claws and interdigital skin and the other a solution of copper sulphate (10 per cent) or formalin (5 per cent). Both copper sulphate and formalin may cause irritation, and for this reason cattle should not be exposed to them more frequently than twice a week.6 A convenient and practical prophylactic programme for dairy cows may be to expose them to a footbath before or after four successive milkings every five days, the footbath being drained and refilled with water between each course of treatment.182 Zinc sulphate as a 10 per cent solution may also be used in a footbath. As it is non-toxic and non-irritating, cattle should be exposed to it daily for the best results.6 However, the effectiveness of zinc sulphate to prevent infectious conditions of the feet in cattle is debatable. Footbaths should be properly constructed to ensure that the feet are exposed to the solution and that the floors are not slippery.182
Formalin or copper sulphate footbaths are rather ineffective on the transmission and development of digital dermatitis lesions.120, 145 Instead, footbaths containing lincomycin or tylosin are frequently used to control herd outbreaks; however, it is important to make sure that cows do not drink such solutions.
Although some studies indicate that the addition of ethylenediamine dihydriodide (at rates of 12.5 to 200 mg/head/day) to the diet does reduce the severity and prevalence of interdigital necrobacillosis in experimental animals,16, 98 others6 determined no such beneficial effects and reported that herds treated with oral iodides for prolonged periods develop a chronic upper respiratory irritation and cough (i.e. signs of iodism).
Zinc supplementation should be considered under circumstances where a zinc deficiency plays a role in the prevalence of interdigital necrobacillosis or other interdigital skin diseases.37
Immunization of cattle against interdigital necrobacillosis with an autogenous D. nodosus vaccine has been used.33 Even though vaccination appeared to decrease the severity of interdigital necrobacillosis, it had only a minor effect on the prevalence of the condition.33
Additional information on the diagnosis, therapy and control of the various conditions of the bovine claw that are discussed in the differential diagnosis may be obtained from the relevant publications.7, 8, 64, 66, 70, 95, 125, 131, 181, 182
Ovine interdigital dermatitis
Introduction
Ovine interdigital dermatitis (OID) is an acute inflammatory condition, mainly of the interdigital skin of the feet of sheep, caused by F. necrophorum in association with Trueperella (Arcanobacter) pyogenes, although other non-specific bacteria may also be involved.122, 188 It is usually accompanied by maceration and erosion of the affected parts. Pitting of the soft horn is occasionally present in severely affected animals. Clinically, benign foot rot closely resembles OID. Dichelobacter nodosus organisms are absent from smears of ovine interdigital dermatitis and this appears to be the main distinguishing feature between these two conditions. Lameness usually occurs in only a small proportion of affected sheep, although it is generally this clinical sign which draws attention to the fact that the disease is present in a flock. In some outbreaks, however, a large number of animals in the flock may become lame. Excessive moisture and heavy faecal contamination of the environment are two of the most important predisposing factors.49, 122 Fusobacterium necrophorum may survive for several months in faecally contaminated, muddy conditions and occurs in the gastrointestinal tract as part of the microbial flora of different animal species.
Aetiology and epidemiology
Ovine interdigital dermatitis, foot abscess, toe abscess and foot rot are distinct infectious conditions of the feet, particularly of sheep and occasionally of goats, which are caused by infections with F. necrophorum and/or D. nodosus in association with other infectious agents such as T.(Arcanobacter) pyogenes. Of these conditions, OID is the mildest, but it may predispose to foot rot and foot abscess, which are much more severe conditions.48, 136
Although foot abscess and toe abscess are often confused with each other and described as though they were the same entity, they are two distinct suppurative conditions with different pathogeneses. Foot abscess is the more common of the two conditions.
The seasonal occurrence of OID in Australia122 and New Zealand,186 and its association with wet conditions following prolonged rainfall are well known. In South Africa, the prevalence of OID is dependent on suitable climatological conditions. It occurs in the coastal area of KwaZulu-Natal and those parts of the Eastern and Western Cape provinces that have a high annual rainfall, but favourable conditions for its occurrence may also develop in other parts of the country during periods of prolonged high rainfall. It may also occur on farms where wet underfoot conditions prevail, such as in the vicinity of leaking drinking troughs, or in poorly drained camps, pens or irrigated pastures.
A number of other factors may also adversely affect the integrity of the interdigital skin and lead to outbreaks of OID. Inadequate dietary levels of zinc, or its unavailability due to mineral antagonism, may result in the formation of a poor-quality interdigital skin and horn which enhances the probability of invasion by F. necrophorum.142 Overgrowth of the horn of the feet, particularly of the walls and heel, which prevents the claws from opening and drying out, tends to trap mud and faeces and keeps F. necrophorum in continuous contact with the feet.13, 109
Differences in breed susceptibility are recognized, with Merinos being most susceptible under conditions of moderate challenge.109 Individuals within breeds may be more than usually susceptible and are prone to successive attacks of OID.
Although all age groups of sheep are susceptible, young animals about eight months of age are most commonly affected. Because of the behavioural patterns of young rams, the pastures on which they are kept are often trampled and the soil becomes and remains muddy. They frequently mount each other, which increases the risk of physical damage to the interdigital skin that predispose them to develop foot abscess188
Apart from the above-mentioned conditions, other diseases may also cause lameness in sheep and goats (see Ovine foot rot: Differential diagnosis).
Pathogenesis
Trauma or maceration of the interdigital skin permits invasion of F. necrophorum.122 Once invasion of the interdigital skin by F. necrophorum has occurred, the dermonecrotic properties of the bacterium establish the infection. Fusobacterium necrophorum produces a leukocidin that is effective in protecting both itself and T. pyogenes against phagocytosis. Conversely, T. pyogenes produces a diffusible growth factor for F. necrophorum so that these bacteria grow synergistically.122
Clinical signs and pathology
Clinical signs of OID are usually absent or mild.110, 122 Sometimes only a small proportion of affected sheep are lame: the signs being particularly evident when underfoot conditions are moist and muddy. If the feet of supposedly unaffected animals in the flock are examined, it will be observed that many of them are also affected. In mildly affected animals, the lesions are characterized by erythema, swelling and, in some cases, erosion of the interdigital skin of one or more of the feet. Severely affected animals, which usually manifest marked lameness, have macerated, eroded, suppurating interdigital tissues and only rarely erosion and pitting of the soft horn.110, 122, 186 Histologically, the epidermis shows superficial necrosis and sloughing of the epidermis, infiltration with numerous neutrophils and invasion with F. necrophorum and other bacteria.122
Diagnosis and differential diagnosis
The feet of as many sheep as possible in an affected flock should be examined after they have been washed and scrubbed clean with a soft brush.188
The clinical differentiation of OID from benign foot rot or early cases of intermediate or virulent foot rot is not always possible. Absence of D. nodosus from smears in OID is the main distinguishing feature and, with time, virulent foot rot progressively under-runs the wall of the hoof if suitable environmental conditions persist. It is usually not difficult to differentiate OID from foot abscess as the former is almost invariably a mild infection limited mainly to the interdigital skin,186 while in foot abscess the deeper tissues are also involved and the affected digit is generally very painful and swollen, especially in the area above the coronet of its abaxial aspect. Pus may drain through sinus tracts in the skin of the coronet and interdigital area.
Lameness in small stock is also associated with other causes (see Ovine foot rot: Differential diagnosis).
Control
Mildly affected animals usually recover spontaneously if they are transferred from wet or muddy to dry pastures. Walk-through foot-bathing at two- to four-week intervals using 10 per cent zinc sulphate or 5 per cent formalin markedly reduces the prevalence of OID. Treated sheep should be allowed to stand on a dry surface to enable the disinfectant to dry on the feet before they are returned to pasture. Severely affected sheep should be treated as potential cases of foot abscess; the parenteral administration of penicillin may prevent spread of the infection to the distal interphalangeal joints.188
While F. necrophorum vaccines have been made and marketed in some countries, there is little published evidence of their efficacy.
Foot abscess
Synonyms: Infective bulbar necrosis, heel abscess
Introduction and aetiology
Foot abscess (Figure 15) is an acute to chronic, purulent, infectious but non-contagious disease of sheep and goats that usually involves a single digit of one of the feet. It usually follows ovine interdigital dermatitis (OID) or trauma of the interdigital skin and is caused by a mixed infection with F. necrophorum and T. pyogenes132, 136, 186 that extends into the distal interphalangeal joint of the affected digit. It also occurs commonly in goats.

The prevalence of foot abscess is usually less than 5 per cent in a flock of sheep, but it is nevertheless an important disease because of the severity of the lesion and because it generally affects the more valuable animals, such as rams and heavily pregnant ewes. Losses in production may occur as a result of the interruption of the breeding programme and of the development of pregnancy toxaemia as a consequence of the severe lameness which is associated with the disease.188
The general bacteriological characteristics of F. necrophorum and T. pyogenes are given in the introduction to the section entitled Anaerobic, Gram-negative, irregular rods and in the Chapter Trueperella pyogenes infections respectively.
Epidemiology
Any damage to the interdigital skin, such as that caused by excessive moisture, sharp stones, thorns, stubble, ticks, the too frequent use of formalin-containing footbaths or the use of too high a concentration of formalin in a footbath may predispose to foot abscess.
Prolonged and continuous wet or moist and muddy conditions in yards or pastures accompanied by stocking densities which give rise to high levels of faecal contamination of the environment are commonly associated with OID, which may subsequently lead to the development of foot abscess. 132, 136, 186 However, in one study in South Africa, no significant correlation between rainfall and the number of abscessed feet of Angora and Boer goats could be established, but there was a statistically significant correlation between the prevalence of foot abscesses and the seasonal abundance of the smooth brown tick (Rhipicephalus glabroscutatum) and the bont tick (Amblyomma hebraeum).99 The trauma of the skin between the claws that is associated with the common attachment site of both these ticks or that of Hyalomma spp. provides an excellent portal of entry for microorganisms such as F. necrophorum and T. pyogenes.
In southern Africa, there are three Rhipicephalus spp. that have a strong predilection for the feet, and sometimes the legs, of sheep and goats, and to a lesser extent of other animals. Ripichephalus glabroscutatum, a two-host tick, is probably the best known of these species. It occurs most commonly in a fairly restricted area of the south-eastern part of the Eastern Cape Province, and its habit of attaching to the feet between the claws often leads to extremely painful lameness in sheep and goats.162 Rhipicephalus lounsburyi,178 previously described as R. follis,163 is a three-host tick. Sheep are the only domestic animals on which its adults have been detected. They attach to the skin of the heels and feet between the claws. Rhipicephalus lounsburyi was first detected in the Dordrecht district but has since also been identified in the Maclear, Aliwal North and Queenstown districts of the Eastern Cape Province, as well as in other parts of the province, such as the Mountain Zebra National Park near Cradock. Other areas where the tick has been detected include the Impendle district of KwaZulu-Natal; the Bontebok National Park near Swellendam in the Western Cape Province, and the Calvinia district in the Northern Cape Province. The adult ticks are most active from May to September. They occur mainly, but not exclusively, in mountainous and hilly areas covered with vegetation ranging from succulent Karoo, Cape shrubland (fynbos) and coastal renosterbosveld to various types of grassland.178 The third species, Rhipicephalus neumanni, also has a three-host life cycle.178 Sheep are the most common hosts of the adult ticks, but they have also been found on Boer goats. Rhipicephalus neumanni is present in southern Namibia, where it has been found in the Bethanien, Luderitz and Keetmanshoop districts. It also occurs in scattered localities in the Karoo of the Northern and Western Cape provinces, such as in the Prieska, Williston, Fraserburg and Victoria West districts, but is probably also more widely distributed in the rest of the Karoo.178
Pathogenesis
Foot abscess usually develops as a complication of OID or trauma of the interdigital skin. The inflammatory process extends from the skin into the subcutis and ultimately into one of the distal interphalangeal joints (coffin joints) (Figure 16). These joints are vulnerable to infection, particularly those on the axial side (interdigital area) of the digit, in which the joint capsules protrude above the coronary borders as the dorsal and volar pouches (Figure 16).188 These pouches are protected only by skin and a small amount of subcutaneous tissue.

During the early stages of the development of foot abscess, the nature of the inflammatory process tends to be necrotic rather than suppurative, hence the term ‘infective bulbar necrosis’.136 At a later stage in the inflammatory process T. pyogenes becomes dominant and suppuration is then evident. The infection in the joints may spread to surrounding tissues, resulting in rupture of the axial collateral and interdigital ligaments and subsequent deformity of the affected digit. Resolution may take many weeks with eventual fibrosis and synarthrosis.
Clinical signs and pathology
An outbreak of foot abscess may start insidiously in a flock and present as sporadic cases of severe lameness, or it may be characterized by the sudden occurrence of a number of lame sheep. Usually, but not invariably, only one digit of one foot is affected.
On examination of the affected foot there is heat, pain and severe swelling in the interdigital area and above the coronary band (Figure 15). As a result of the swelling the affected digit becomes displaced abaxially (laterally). Blood, necrotic material and pus, which is often creamy-white, are discharged from sinus tracts which usually break out in the interdigital area, although occasionally they may open in the skin at one or more points above the coronet. In about 50 per cent of cases infection of the joint results in rupture of the axial collateral ligaments and the interdigital ligament, giving rise to exaggerated movement of the affected digit, displacement of the digit during locomotion, and permanent deformity. Healing is slow and takes from about two to four months. The development of excessive granulation tissue frequently occurs in the skin and subcutis, especially at sites where the sinuses discharge into the interdigital space. In severely affected animals neighbouring joints may also be affected, and the inflammatory process may extend along the tendons to the fetlock region or even higher.71, 185
Diagnosis and differential diagnosis
The initial lesions of foot abscess are clinically indistinguishable from OID and the earliest lesions of the different forms of foot rot. In general, foot abscess differs from foot rot in that the lesions in the latter disease only involve the interdigital skin and the matrix of the hoof, while in the former, the distal interphalangeal joint and, in some, the associated ligaments and tendons are affected. Foot abscess is almost invariably restricted to one digit of one foot, while foot rot usually affects more than one foot. In foot abscess, the characteristic odour associated with D. nodosus infection is not present, and the prevalence rarely exceeds 5 per cent. Radiology is useful in establishing the involvement of the distal interphalangeal joint in cases of foot abscess.188 Other distinguishing features are given in Table 4.
Control
Treatment of foot abscess should include cleansing of the lesions with disinfectants, drainage of the infected area, and parenteral administration of antimicrobial drugs. Penicillin alone or in combination with streptomycin is effective against F. necrophorum and T. pyogenes. Early cases, before or very soon after the infection reaches the joint, may benefit from aggressive antimicrobial therapy. Nevertheless, eventual recovery cannot always be ascribed to the treatment used, as resolution of infection occurs in most animals after two to four months although the affected digit may be deformed.185 The prognosis is therefore usually good if animals can be given supportive treatment in the form of rest, shelter and hand-feeding until the disease has run its course.
Control is based on minimizing the factors which predispose to OID. Footbaths containing 5 per cent formalin or 10 per cent zinc sulphate used at weekly intervals, may lower the prevalence of OID. The use of too high a concentration of formalin, however, may have the opposite effect and actually increase the prevalence of foot abscess as it causes drying and cracking of the interdigital skin.187 Where the bites of ticks are incriminated as the predisposing factor, tick control using acaricides which are applied in the form of either a footbath or spot treatment of the feet, should be instituted.
Table 4 Comparison of the most important clinical aspects of foot rot, foot abscess and toe abscess in sheep. (Adapted from Walker179)
| FOOT ROT | FOOT ABSCESS | TOE ABSCESS | |
|---|---|---|---|
| Primary infectious agents involved | D. nodosus and F. necrophorum | F. necrophorum and T. pyogenes | F. necrophorum and T. pyogenes |
| Swelling | None | Usually above coronary band | None |
| Exudate | No pus; greyish-black slimy substance may be present | Discharge of creamy-white pus | Blackish pus and gas bubbles may be evident when exposed |
| Odour | Putrid odour. Lesions may be fly-blown | Slight odour. Lesions are rarely fly-blown | Odour distinct from that of foot rot. Lesions may be fly-blown |
| Sheep affected | All ages under conditions favourable to its development | Usually confined to heavy animals, e.g. rams and pregnant ewes | All classes of sheep |
| Location of lesion | No break in the skin of the coronet but separation of the inner sensitive horn from the outer hard horn | Sinus tracts usually break out at the coronet or the interdigital skin | Usually under horn of toe. May open in a line above coronary band but usually needs to be exposed by paring |
| Hoof | Often markedly misshapen | Usually normal | Slight distortion over the lesions |
Toe abscess
Synonym: Lamellar suppuration
In toe abscess,it is presumed that in most cases infection gains entry through minute fissures in, or trauma to, the horn of the hoof, especially at the sole-wall junction (white line).188 The toe of one digit of a fore foot is usually involved. Sheep with misshapen or overgrown hoofs, or those whose hoofs have been subjected to injudicious paring, are particularly prone to toe abscess. However, toe abscess is an uncommon condition. In contrast to the association between foot abscess, foot rot and ovine interdigital dermatitis, the latter is not involved in the pathogenesis of toe abscess.
Toe abscess is caused by a mixed infection of bacteria, in which F. necrophorum predominates. Arcanobacter T.pyogenes is also commonly implicated as one of the pathogens.171
The earliest sign of toe abscess in a flock of sheep is the appearance of acute lameness affecting one limb of one or more sheep. These animals tend to ‘carry’ the affected leg as a result of the severe pain. In the early stage of the disease, clinical examination may fail to reveal any obvious lesion, although one claw is generally found to be hot and painful on palpation. Careful paring away of the horn at the toe will, however, reveal the presence of greyish pus of fairly thick consistency in the affected part. In more advanced cases, the suppurative process may be found to have spread posteriorly under the sole, or to have ‘broken out’ to the externum through sinus tracts above the coronet. Because it primarily affects the lamellae of the hoof it is also known as ‘lamellar suppuration’.
Toe abscess must be distinguished from foot abscess and foot rot (Table 4). It should also be differentiated from the condition known as shelly toe (also referred to as shelly hoof, white line disease), a non-infectious disease characterized by separation of the hoof horn from the sensitive laminae. The cavity that forms as a result of the separation is often packed with debris. The condition seldom causes lameness. The therapy for toe abscess consists of exposing the lesion and treating it as an open wound. Parenteral antimicrobial therapy is indicated.
Ovine foot rot
Introduction and aetiology
Foot rot is a highly contagious, painful and debilitating bacterial disease, particularly of sheep, usually affecting more than one foot. It is caused primarily by synergistic infection with Dichelobacter (Bacteroides) nodosus and Fusobacterium necrophorum. Other organisms, such as Arcanobacter T.pyogenes and Spirochaeta penortha, are often isolated from affected feet, but they do not play a primary role. The intact interdigital skin is a strong barrier to D. nodosus. In almost all cases of foot rot there is predisposition from ovine interdigital dermatitis and F. necrophorum infection resulting in damage to the interdigital skin.48, 49 As a result, environmental factors, such as wet, muddy conditions, are important predisposing factors to foot rot, but other factors may also be involved.55, 109, 134 An outbreak in a flock is usually heralded by the presence of a few limping sheep as a result of the disease, which may rapidly spread to affect a large proportion of sheep if environmental conditions are suitable. Based on the severity of the lesions, three forms of foot rot are recognized — benign (non-progressive, mild), intermediate, and virulent (progressive). The severity of the disease depends on the virulence of the infecting strains of D. nodosus, the resistance of the host, and environmental factors.22 Cattle may be carriers of benign strains of D. nodosus. These strains cause interdigital dermatitis in cattle if suitable conditions prevail.
Foot rot is a common, economically important disease in Australia, New Zealand, the USA, the UK and other countries in Europe. The first isolation of D. nodosus in South Africa was made only in 1984,14 from foot rot lesions of sheep in KwaZulu-Natal, but clinical cases of what was probably foot rot in sheep and goats have been recognized for many years in South Africa.165, 170 Subsequently its presence has been confirmed in cases of foot rot in sheep in several provinces of South Africa.
Foot rot is an important disease because it causes losses in production as a result of reduced body and fleece weights, decreased length and tensile strength of wool fibres, and reduced fertility (due to loss in bodyweight). The lesions are prone to blowfly strike which aggravates the effects of the disease.13, 155, 156, 179 The labour and costs involved in control programmes contribute further to its economic importance.
Consult the introduction to the section entitled Anaerobic, Gram-negative, irregular rods for information on the general characteristics of D. nodosus and F. necrophorum.
Epidemiology
Dichelobacter nodosus is an obligate parasite of the skin of the feet of sheep, goats, cattle and deer.154 It cannot survive in the environment for more than seven days,3 and infected animals, particularly sheep, are the main reservoir of infection. A proportion of sheep are “carriers” of D. nodosus, which persists in small pockets in the sole or wall of the hoof during unfavourable environmental conditions. These pockets are detectable if individual feet are examined, but the sheep are not lame and so from a clinical point of view may be considered asymptomatic “carriers”. They may remain infected for four to six months or longer, and then may develop overt foot rot if conditions become favourable, resulting in further spread of the infection. They therefore pose a threat to eradication programmes.21, 179 Cattle may also be a source of benign foot rot in sheep as they are frequently infected with strains of D. nodosus that cause benign foot rot. Benign strains have also been isolated from farmed deer in Australia and New Zealand.179 This is one of the reasons why benign foot rot may occur on properties from which virulent foot rot has been eradicated, or may be due to the survival of benign strains despite successful elimination of virulent strains.5 Benign strains of D. nodosus are more difficult to eradicate from flocks than virulent strains as they may be present in healthy interdigital skin, making some infected sheep very difficult to detect.3 Benign foot rot may also be introduced following the introduction of apparently healthy sheep, goats or cattle infected with D. nodosus strains of low virulence.156, 179
Fusobacterium necrophorum is part of the normal microflora of the intestinal tract of ruminants and may therefore occur in the environment through faecal contamination. It may survive for several months in faecally contaminated, muddy conditions.84, 94, 137, 149
Prolonged wet and muddy conditions with ambient temperatures above 10 °C are the most important factors that contribute to the transmission of D. nodosus and the spread of foot rot.62 Other predisposing factors include traumatic injury to the interdigital skin, such as that caused by the penetration of Strongyloides papillosus larvae,21 grasses, such as kikuyu (Pennisetum clandestinum), and thorns, as well as hoof cracks and over-grown hoofs, which increase the susceptibility of the feet to bacterial invasion.142
Merinos are more susceptible to virulent foot rot than British breeds, but there is individual variation in susceptibility within breeds;52 horn quality and the degree to which the claws can spread seem to be the major determining factors. All ages and both sexes of sheep are susceptible.
Pathogenesis
Foot rot starts as an infection of the interdigital skin which, depending on the form of disease (benign, intermediate or virulent, with virulent being the most progressive), then progressively spreads down the inside of the inner (medial) wall of the hoof and across the sole, causing under-running and separation of the horn (Table 5). In very severely affected animals, the infection also extends from the sole up the outer (lateral) wall of the hoof. The severity of the disease is mainly determined by the virulence of the strain of D. nodosus involved, but environmental factors (e.g. temperature, moisture) and breed of sheep also play a role.179
Table 5 Scoring of lesions of sheep suffering from foot rot. Adapted from Walker179
| SCORE | LESIONS |
|---|---|
| 0 | Normal, dry interdigital skin |
| 1 | Mild, localized interdigital dermatitis; slight to moderate inflammation which includes erosion of the epidermis |
| 2 | Moderate interdigital dermatitis and necrotizing inflammation of part or all the soft horn of the medial wall of the digit |
| 3 | Severe interdigital dermatitis and under-running of the horn of the heel and sole; the necrotizing inflammation does not extend to the outer edge of the sole |
| 4 | Under-running extending to the outer edge of the sole of the hoof |
| 5 | Necrotizing inflammation of the deeper layers of the hoof, resulting in separation of the hoof |
In foot rot, F. necrophorum is critical for initial tissue destruction. Dichelobacter nodosus enhances the infection by producing a growth factor which enables F. necrophorum to multiply in the deeper parts of the lesion. In these areas D. nodosus grows slowly but persistently and prevents healing during periods when F. necrophorum is quiescent. The pili of D. nodosus allow the bacterium to adhere to the epidermal matrix of the horn while the protease it produces digests the horn, thus promoting its separation and facilitating invasion by other species of bacteria. The latter aggravate the lesion and help to provide the anaerobic conditions which enable D. nodosus and F. necrophorum to grow.
Clinical signs and pathology
The severity of lesions of foot rot in sheep may be scored (Table 5) in order to differentiate the three forms of foot rot and also as an aid to decide which control programme should be implemented.
In benign foot rot, sometimes also referred to as ‘scald’, the majority of lesions are Score 2, with the interdigital skin lesions being characterized by hyperaemia, moistening and, in some, granulation tissue formation. The lesions rarely progress to an under-running of the horn (Score 3 or 4). There is often ridging of the horn on the medial posterior wall in more chronic cases. Usually more than one foot is affected. Many animals in a flock may be affected under conditions favourable to the spread of foot rot. Most cases of benign foot rot resolve without treatment if animals are moved to dry pastures and the lesions usually do not become chronic. It has a minimal effect on production of meat and wool.156, 179
Next in order of severity of lesions is intermediate foot rot. These lesions usually develop more slowly than those of virulent foot rot (Table 6). The severity of lameness is commensurate with the severity of lesions. A variable proportion of the flock may be affected. Up to 10 per cent of sheep may have lesions with a Score of 4. Self-cure of most affected animals may occur if environmental conditions become drier.
Virulent foot rot spreads rapidly in a flock; under ideal environmental conditions for the development of foot rot, up to 90 per cent of a flock may become infected within six weeks. Affected sheep are severely lame and lose weight. The disease commences as an interdigital dermatitis but the subsequent lesions develop rapidly, and in one to two weeks (Table 6) there is severe under-running of the hoof (Figure 17). At least 10 per cent of affected sheep have Score 4 lesions and the proportion is frequently much higher. In a proportion of cases with virulent foot rot do the lesions resolve spontaneously as environmental conditions become drier, but many sheep develop chronic lesions. Sheep suffering from chronic virulent foot rot often have overgrown and misshapen hoofs, while the soft tissue beneath the horn is destroyed and may have a greyish-black, tarry appearance (Figure 18). Myiasis of the lesions may occur, and this compounds the severity of the disease.
Both virulent and benign strains of D. nodosus have been isolated from goats with foot rot.179 The predominant lesion in goats is severe interdigital dermatitis characterized by hyperkeratosis, erosions and necrosis, with only occasional under-running of the sole. Some granulation tissue formation may accompany the interdigital dermatitis. Severely affected goats may exhibit marked lameness and weight loss. 156, 179
Diagnosis and differential diagnosis
Visual and manual inspection of all the feet of as many sheep as possible is the most practical way of diagnosing foot rot.44 An enzyme-linked immunosorbent assay (ELISA) has been developed to detect infected flocks during periods when the disease is subclinical.191 Protease tests (gelatin gel thermostability test, elastase test) and PCR tests have been used, but it is important that sufficient samples are collected to ensure the D. nodosus isolates recovered contain the most virulent isolates. A retrospective assessment of the presence and severity of clinical disease is possible with an anamnestic test in which sheep receive a subcutaneous injection of an antigen from D. nodosus.190 However, these tests have lacked specificity, especially in older sheep. The lesions should be graded and scored 0 to 5 to determine which form of foot rot is prevalent in the flock (Table 5). Severe under-running of the hoofs in a large proportion of sheep will indicate virulent foot rot. Benign foot rot is characterized generally by interdigital lesions with little under-running, even under suitable environmental conditions. The severity of the lesions of intermediate foot rot is between those of virulent and benign foot rot.
If foot rot is suspected and environmental conditions are not favourable for its development, the ‘progression test’ is a useful diagnostic aid. In this test, 10 to 20 sheep with score 2 to 3 lesions are identified and placed on wet rubber mats, wet straw or irrigated pastures at ambient temperatures above 10 °C for seven days.179 After one to three weeks the lesions are reassessed, and if they have progressed rapidly a diagnosis of virulent foot rot is justified.
Microscopic examination of smears prepared from material obtained from interdigital skin lesions or other active lesions, such as the margin of the most recent under-run part of a hoof or an active lesion that has been exposed by paring, may be used to determine the presence of D. nodosus. However, this is not useful to determine the type of foot rot present.
The smears should be stained with the Gram’s staining method or a fluorescent antibody staining technique. The rod-shaped bacteria have characteristic terminal enlargements. False negative results by both these methods are sometimes obtained when recently treated sheep are examined or at times of the year when unfavourable conditions for the multiplication of the bacteria prevail.179
Table 6 Time-scale of development of lesions of foot rot in sheep. (Adapted from Walker179)
| LESIONS | TIME SCALE | ||
| BENIGN | INTERMEDIATE | VIRULENT | |
| Interdigital dermatitis | 3–4 days | 3–4 days | 3–4 days |
| Separation of the skin/horn junction at heel (score 3) | 30 days | 7–14 days | |
| Separation of entire sole to outside wall (score 4) | 21 days | ||
| Chronic infection | Months | ||
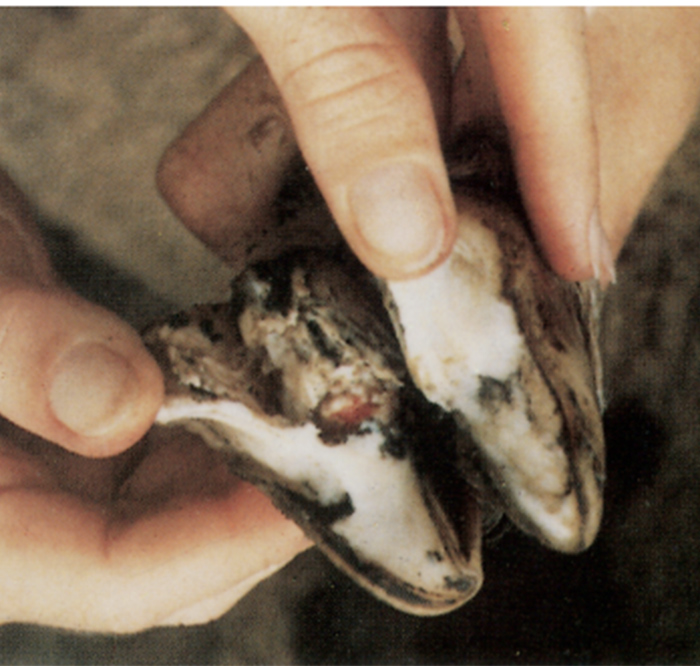
Culturing of D. nodosus from active lesions can be attempted. The best results are obtained if material from the lesions is inoculated onto plates containing a specialized medium known as hoof agar. The plates are immediately placed in an anaerobic jar and sent to a laboratory familiar with culturing D. nodosus.179 Alternatively, special transport media should be used. Once D. nodosus is isolated, its virulence and the serogroup to which it belongs can then be determined. For information on the morphological characteristics and cultural requirements of D. nodosus, as well as its identification, consult the introduction to the section entitled Anaerobic, Gram-negative, irregular rods
Foot rot is most commonly confused with foot abscess. Some characteristics that will help to differentiate foot rot, foot abscess and toe abscess from one another are summarized in Table 4. Other causes of lameness in sheep include injury or trauma to the feet (such as those caused by thorns of Tribulus terrestris or ‘dubbeltjies’ and tick bites) or joints of the legs; orf lesions around the coronet, heels and in the interdigital skin; coronitis caused by bluetongue; post-dipping lameness caused by Erysipelothrix rhusiopathiae; polyarthritis due to a variety of infectious agents; laminitis due to feeding of excessive amounts of carbohydrates; and white muscle disease (nutritional myopathy).

Control
The economic benefits of control (reducing the prevalence of ovine foot rot to an acceptable level) versus elimination (eradication) strategies should be discussed with the flock owner, and the expected extent of his or her co-operation assessed, before any programme is implemented.2, 44
In the case of virulent foot rot in susceptible breeds of sheep, implementation of an elimination strategy is usually indicated, but control may be the best option where the prospects for elimination are poor. If control is the objective, vaccination or foot-bathing will reduce the prevalence of virulent foot rot in a flock.44, 135 Once the prevalence has been reduced to a low level, its elimination may become feasible. Where benign foot rot is the problem, control should be attempted during the wet seasons, as the elimination of it is difficult. In the case of intermediate foot rot, an elimination strategy of the disease in young sheep may be undertaken initially, and if successful could be expanded to include the other age groups.2
Various methods may be applied to control foot rot. These include the removal of affected flocks from wet pastures to dry areas, parenteral or topical antimicrobial therapy, foot-bathing and vaccination.6, 179 Paring of affected hoofs to expose pockets of infection has previously been suggested prior to topical or parenteral antimicrobial therapy or foot-bathing, but it is very time-consuming and thus expensive. Depending on the situation on the farm, one or more of these methods could be combined. Preventive measures (foot-bathing and vaccination) are applied before or during wet conditions which favour transmission,4 while therapeutic measures (antimicrobial therapy and paring) are most effective during dry conditions (the non-transmission phase).44
Walk-through foot-bathing should be instituted during the transmission periods in order to reduce the prevalence of overt disease in carriers which may exist.179
The preparations used in footbaths are usually 10 per cent zinc sulphate, 5 per cent formalin, or commercial products (e.g. Footrite; Hardman Chemical (Pty) Ltd) which contain zinc sulphate and sodium lauryl sulphate, the latter enhancing penetration of zinc sulphate into the hoof.10, 29, 76 Portable or permanent troughs may be used as footbaths; the former can be placed, for example, in gateways. Fresh solutions should be made up regularly. Generally, control of benign foot rot and most cases of intermediate foot rot is satisfactorily effected if animals walk through, or preferably, stand in the footbath for up to five minutes every two to four weeks to ensure that all four feet are treated. Sheep should stand on dry areas for 10 to 20 minutes following foot-bathing to allow the solution to dry on the feet so that the chemical it contains will have a lasting effect. The principle of a walk-through foot-bathing programme is that the chemical used makes contact with the interdigital skin and the area of under-running so that D. nodosus is killed.
Vaccination or more intensive foot-bathing (weekly ‘walk-through’, or ‘stand-in’ every two to three weeks) prior to or during the transmission period will be required to control virulent foot rot.2 With Footrite, which contains both zinc sulphate and sodium lauryl sulphate, the interval could be up to 21 days between treatments.179 A high cure rate is usually obtained with it without prior paring.29
Parenteral antibiotics have also been used to treat sheep with foot rot. A single intramuscular injection of penicillin/streptomycin at a dosage rate of 70,000 IU/kg procaine penicillin and 70 mg/kg dihydrostreptomycin achieved cure rates of 78 to 100 per cent in sheep under dry conditions, and 42 to 63 per cent when sheep were returned to wet pastures.47 Parenteral chemotherapy has the advantage of not requiring the extensive paring which is a prerequisite for effective topical treatments.173 Antibiotic levels increase in lesions under dry conditions which may explain the range in cure rates. Concurrent supportive treatment of trimming under-run horn and 5 per cent formalin foot-bathing increases the efficacy of antibiotic therapy.
Other antibiotics have also been used to treat foot rot, including a mixed solution of 50 mg lincomycin and 100 mg spectinomycin/ml given at a dosage rate of 1 ml/10 kg,177 erythromycin at 8 to 10 mg/kg,184 and oxytetracycline at 20 mg/kg body weight.133 When used as a once-only injection these antibiotics have achieved similar cure rates to penicillin/streptomycin treatments. Parenteral antibiotic therapy has been widely used to treat foot rot in Australia,184 although there are concerns about the treatment of large numbers of sheep with relatively high doses of antibiotics. Some chronically affected sheep do not respond to antimicrobial treatments and should be culled.179
Various inactivated adjuvanted (mostly oil) vaccines containing different strains of D. nodosus serogroups have been commercially available in Europe, Australia and New Zealand. The use of vaccines gives a farmer an alternative method for the control of foot rot in wet conditions other than simply foot-bathing.44 Vaccination is used to reduce the prevalence of foot rot in flocks to manageable levels and it has the advantage that it is less labour intensive than footbathing. Vaccination not only induces immunity which prevents the infection from becoming established in 80 per cent of sheep, but it also has a curative effect; the lesions resolve in at least 60 per cent of affected sheep that are vaccinated.44, 179 Once the prevalence of foot rot in a flock has been reduced through vaccination, elimination could be attempted either by disposal or chemotherapy of affected sheep.44
Depending on the make of the vaccine, the interval between the administration of the first and second dose of vaccine varies, but it is generally at least two weeks.44, 135 An effective immunity develops only after the second dose of vaccine, and maximum protection lasts for only 10 to 12 weeks after administration of the second dose. The administration of a single booster dose of vaccine prior to the wet season in the subsequent year will provide good protection.135, 179 The vaccination programme should be planned so that maximum protection occurs during the period that the prevalence of foot rot is most likely to be increasing.135, 179 Vaccinated ewes confer colostral immunity to their lambs, and maternal antibodies may interfere with the response of vaccination in lambs less than eight weeks of age.135
Dietary zinc has been claimed to improve the quality of the horn of the hoof and interdigital skin and therefore decreases the susceptibility of sheep to infection.142 However, various studies using different dosage rates of zinc have failed to demonstrate any benefit in reducing the prevalence or severity of D. nodosus infections, or in enhancing the resistance of sheep to foot rot.46, 132, 184
Several strategies can be applied to eliminate virulent foot rot. 44, 179 The basis of elimination of virulent foot rot is that D. nodosus does not survive for prolonged periods except in sheep or goats’ feet, and that infected animals can be detected clinically, allowing the identification of all infected animals. Methods that can be applied to achieve elimination of foot rot fall into three categories:44
- disposal of the entire flock and restocking with sheep free of foot rot;
- identification and disposal of affected sheep in a flock; and
- elimination of infection by chemotherapy, either most commonly by identification of infected sheep and chemotherapy of those sheep, or in specific cases, chemotherapy of the whole flock.
Sheep free of foot rot should be identified and isolated from infected sheep, while the infected ones are either treated or culled. The best results are generally obtained if elimination is attempted during the dry summer months when transmission of foot rot is unlikely. The use of antibiotics to treat infected sheep is also more efficacious under dry conditions. Elimination of foot rot can be achieved in a single season, but for many producers elimination is not always successful in the first year and it is more common for elimination to take two to three years. The reasons for failing to eliminate foot rot include inadequate control during the transmission period, leading to too many infected sheep to deal with, operator error, incomplete musters and short “dry” seasons.108
More recently, vaccination using monovalent and bivalent recombinant vaccines has lead to elimination of virulent foot rot in some flocks.39, 45, 72 For this strategy to be successful and a practical alternative to inspection and culling or treatment, the outbreak of foot rot needs to be associated with few different serogroups – ideally two or less. Inspection and culling of non-responders is still necessary. The advantage of this approach is that it is less labour intensive and less dependent on seasonal conditions. In general, monovalent whole cell vaccines are rather inefficient as they do not confer adequate cross-protection against heterologous serogroups. Therefore, in situations where mono- or bivalent vaccines appear to be performing poorly, using a commercial custom-made vaccine, which targets the exact strains of foot rot bacteria identified in individual flocks, as is presently done in Australia, may be the best approach.38
Any elimination strategy must incorporate regular surveillance of the flock after affected sheep have been removed.44
Bovine hepatic necrobacillosis
Synonym: rumenitis-liver abscess complex
Introduction
In cattle there is a close association between rumenitis and the development of hepatic necrobacillosis (liver abscesses). Infection of the liver usually originates from a necrobacillary rumenitis.113 In many cases Fusobacterium necrophorum, particularly biovar A, may be isolated in pure culture from these lesions, but more often the infection is mixed, Trueperella (formerly Arcanobacter) pyogenes being the most common bacterium to accompany F. necrophorum. The lesion in the liver produced by uncomplicated F. necrophorum is frequently described as an abscess, but this is not so if the strict definition of the term is applied. Fusobacterium necrophorum causes localized areas of hepatic necrosis which are initially coagulative in nature. The necrotic tissue may later undergo liquifaction and/or become invaded by pyogenic organisms and may then resemble pus, making the lesion as a whole to look like an abscess (see Clinical signs and pathology). Nevertheless, in order to follow general practice the term ‘abscess’ is used in this section.
Hepatic necrobacillosis or the rumenitis-liver abscess complex in cattle, which occurs most frequently in feedlot animals,78, 79, 101, 105, 113, 116, 143 may cause considerable economic loss, primarily because of the condemnation of affected livers at slaughter. In some animals, the liver lesions result in acute or chronic systemic disease. Surveys conducted in the USA between 1967 and 1969 indicated that approximately 10 per cent of cattle slaughtered had abscesses in their livers. However, abscesses only occurred rarely in other organs. Publications 2 decades or so later indicate an abscess prevalence of 20 to 30 per cent in feedlot cattle.69, 73
More recently, the prevalence of liver abscesses in feedlot cattle in Australia and the USA was reported to range from 1 to 2 per cent to as high as 90 to 95 per cent, with up to 40 per cent of livers from feedlot cattle condemned at slaughter.176
Abscessation of the liver is also seen with increasing frequency in dairy cattle fed grain (i.e. rations that predispose to rumenitis), as well as in pasture-fed cattle, possibly associated with the high sugar content of lush spring pasture (as much as 50 per cent of the dry matter).176
Aetiology
Hepatic abscesses are usually polymicrobial infections, with anaerobes being the predominant organisms and F. necrophorum the primary aetiological agent. Fusobacterium necrophorum can be isolated in pure culture from 81 to 97 per cent of small or newly formed hepatic abscesses in cattle.85, 101, 116, 148 As the abscesses increase in size and age, they usually become secondarily infected by one or more of a variety of anaerobic or facultative anaerobic bacteria.
Biovars A, B and AB of F. necrophorum are usually associated with hepatic abscesses.1, 17, 85, 87 Strains of biovar A (F. necrophorum necrophorum) are usually isolated in pure culture from liver abscesses17, 85, 148 and may be isolated from as many as 50 per cent of all cases.96 These biovar A strains have a greater potential to cause liver abscesses, which is attributed to virulence factors in their cell walls and the production of more leukocidin than the other two biovars.56 Strains of biovar B (F. necrophorum funduliforme) are most often isolated from micro-abscesses in the rumen.87 Biovar B strains are less virulent than biovar A and they invariably occur in association with other micro-organisms, particularly T. pyogenes and Bacteroides spp., on which they depend to exert their pathogenic effects.17, 96 Biovar AB strains are rarely isolated and their pathogenicity is intermediate between those of biovars A and B96 (see Epidemiology and pathogenesis).
For further information on the general characteristics of F. necrophorum, consult the introduction to the section Anaerobic, Gram-negative, irregular rods
Epidemiology and pathogenesis
Fusobacterium necrophorum is part of the normal bacterial flora of the alimentary tract, especially the rumen, of healthy cattle.59, 84, 137, 148 It does not penetrate normal intact epithelium; devitalization of the tissue is essential if this is to happen.51 The concentration of F. necrophorum in rumen contents is normally low, but it increases dramatically when the diet is changed from roughage to high-grain.176 Because F. necrophorum uses lactate as its major energy substrate, the increased population in cattle on such diets is probably due to the increased availability of lactate in the rumen. Necrobacillary rumenitis is usually the result of rapid intra-ruminal fermentation of dietary carbohydrate (whatever the source), with subsequent production of lactate and increased acidity of the rumen contents.176
The prevalence of liver abscesses is highest in cattle that pass through feedlot systems. In order to appreciate the reason for this phenomenon, it is necessary to understand the processes involved in the adaptation of these animals to the nutrition they receive while in the feedlot. The intense economic pressure to move these animals through the system as quickly as possible is opposed by several biological constraints. Most cattle entering a feedlot have come from open grazing systems, where the most, if not all, of the animals’ feed intake consisted of high-fibre veld or pasture grasses. Since few cattle in Africa are grazed on mixed pasture, some of which may contain the more digestible clovers, most of them are adapted to a diet containing a large proportion of fibre and little soluble carbohydrate. As a result, the physiology and ecology of their digestive tracts are adapted to optimize the fermentation and digestion of the cellulose and hemicellulose fractions of the diet. In other words, the rate of passage of digesta through the tract will be slow, the retention of particles in the rumen will be long, the volume of saliva will be copious, but it will not contain much bicarbonate, and the cellulolytic and hemicellulolytic micro-organisms will be well represented in the rumen ecology, while lactolytic groups will be present in only small numbers.
In principle, it is possible to adapt cattle from the more natural high-fibre diet to one containing very little fibre (as little as 10 to 20 per cent) and large quantities of highly digestible carbohydrates, such as starch. This adaptation results in an increase in the rate of passage of digesta through the digestive tract, which includes a considerable shortening of the retention time of digesta in the rumen, and the production of more bicarbonate in the saliva. In addition, extensive population changes must occur in the rumen ecology if an animal is to cope with this change in substrate. There are always groups of micro-organisms, containing bacteria such as Selenomonas ruminantium and Streptococcus bovis, which can rapidly ferment soluble carbohydrate, thereby producing small amounts of lactate as end-product.140 This lactate is then rapidly transformed to propionate by the lactolytic group of micro-organisms, which include Veillonella parvula (V. alcalescens), Megasphaera elsdenii and S. ruminantium.100 However, when the influx of soluble carbohydrate increases suddenly, as often happens when cattle are first introduced to a feedlot diet, several factors combine to exacerbate the situation. Firstly, reduced tactile stimulation of the rumen wall by grass particles leads to a reduction in saliva production and hence in its buffering capacity. Secondly, the amount of lactate produced in the rumen from the soluble carbohydrate is more than the lactolytic bacteria are able to metabolize, and this hydroxy acid then accumulates in the rumen. The Gram-positive Strep. bovis and other lactobacillus spp. normally produce acetate, propionate and ethanol as end-products at low growth rates, but switch to lactate production at high growth rates.140 As a result, the pH in the rumen declines rapidly from the normal range of 6.5 to 7.2, to 4.5 to 6.5, because lactate (pKa = 3.73) is a stronger acid than are the volatile fatty acids (pKa = 4.76 to 4.82). This decline in pH suppresses several important groups of micro-organisms in the rumen, including those that ferment the fibre component of the diet, as well as those responsible for removing the excess lactate. However, the low pH in the rumen does not have an effect on F. necrophorum. Rumen acidosis, if it is not fatal in itself, may persist in a subacute form, with the acid contents of the rumen producing areas of superficial necrosis of the ruminal epithelium or even in a low-grade rumenitis.78 Fusobacterium necrophorum alone or with other bacteria then colonize these lesions in the rumen wall.
The areas of the rumen affected are usually located in the cranial ventral sac,78 and if they are invaded by F. necrophorum, the destructive effect of leukocidin produced by the organism on the plasma membrane of ruminal epithelial cells increases the severity of the lesions.86
Once F. necrophorum has penetrated the rumen wall, bacterial emboli may enter the hepatic portal circulation, seeding bacteria throughout the liver.79, 113 The bacteria then readily proliferate in the liver tissue and form abscesses.
Infection by F. necrophorum alone may result in liver abscessation, but it does appear that the chances of establishing the infection in the liver are enhanced by a number of factors. Endotoxin released in the rumen during rumen acidosis from the outer cell wall of dying and disintegrating Gram-negative bacteria may contribute to the development of hepatic abscesses41, 112, 166 by impairing the phagocytic ability of cells in the liver, initiating disseminated intravascular coagulation, and causing focal hepatic necrosis.91 Based on experimental data, it appears that most of these effects are mediated through the Schwartzman reaction.114, 115 In addition to the effects of endotoxin in the liver, platelet aggregation mediated by haemolysin and a toxic metabolite of F. necrophorum88 also predisposes to the development of hepatic necrosis.83, 114 Once the bacteria have lodged in the liver, the synergistic effect of toxic substances produced by them causes enlargement of the areas of necrosis.114
It has been shown experimentally that the development of liver abscesses caused by F. necrophorum is enhanced by the presence in the lesion of sub-lethal numbers of T. pyogenes.159 Thus the minimal intravenous infective dose of F. necrophorum required for the causation of liver abscesses may be reduced from more than one million organisms to less than ten. Other bacteria that are able to fulfil the role of so-called ‘helper agent’ include Staphylococcus aureus, Bacillus cereus and Klebsiella oxytoca. The ability of Bacillus subtilis, Mannheimia (formerly Pasteurella) haemolytica, Proteus mirabilis,151, 152 Citrobacter freundi, alpha haemolytic streptococci and Bacillus fragilis to help in the formation of these lesions is less developed.150
In addition to rumen acidosis, foreign objects, such as pieces of wire, nails and other metal or sharp fragments, that are inadvertently ingested with the feed, may also cause injury to the rumen wall (especially the reticulum) and therefore also provide portals of entry for F. necrophorum57, 80 or other bacteria. Disseminated liver abscesses may also be caused by direct extension from umbilical infections in new-born calves, and as a consequence of bacteraemic diseases.113, 176
The infectivity of F. necrophorum appears to be enhanced by faecal contamination of wounds. It has been shown experimentally that the addition of F. necrophorum to a suspension of faeces reduces the minimal infective dose of the organism when the suspension is injected subcutaneously. A similar outcome may be obtained when F. necrophorum is inoculated into a subcutaneous site in which faecal material has previously been injected. Fusobacterium necrophorum may metastasize from the liver to the lungs where similar lesions can then develop.80
Clinical signs and pathology
In most cases, hepatic abscesses are too small to produce overt clinical signs and are usually only detected at slaughter or at necropsy. Occasionally, however, systemic disease or even fatality results when the number of abscesses in the liver is large enough to cause hepatic insufficiency or toxaemia, or when an abscess ruptures which is then followed by peritonitis.80 Cattle with ruptured liver abscesses may be severely depressed, anorexic and febrile.
When large numbers of abscesses develop simultaneously, affected cattle may show periodic fever, inappetence, depression and evidence of pain (i.e. when pressure is applied to the xiphoid process of the sternum or the posterior rib cage on the right side of the animal), while some affected animals may be icteric.80 Feedlot cattle with abscesses have reduced feed efficiency, and those with severely abscessed livers may have a 15 per cent reduction in liveweight gain compared with cattle with no abscesses.113, 176
Single or multiple abscesses of varying size may be present in the liver. They may be located deep in the parenchyma or close to the capsule; in the latter case the inflammatory reaction may involve the capsule of the liver and cause a localized perihepatitis. Most liver abscesses are occult lesions that over time regress to form a sterile scar. Those that progress to proper abscesses are initially pale yellow and are spherical with irregular outlines. The lesions from which pure cultures of F. necrophorum are isolated characteristically consist of round, raised or sunken areas of dry coagulation necrosis of the hepatocytes (Figure 19) which may be surrounded by a zone of intense hyperaemia and inflammation. Older abscesses have a core that is progressively encapsulated by fibrous connective tissue. They are usually 4 to 6 mm in diameter, but occasionally much larger. Peritonitis may be present if an abscess has ruptured into the abdominal cavity, and the liver may be adhered to the diaphragm with fibrous connective tissue.
Histologically, the earliest lesions are micro-abscesses, possibly induced by emboli of F. necrophorum in the sinusoids, which then progress to areas of coagulation necrosis. The peripheral rim of the necrotic lesion contains scattered basophilic debris of nuclear material among which numerous filamentous, non-branching, granular, Gram-negative F. necrophorum organisms are visible. The inflammatory reaction is principally mononuclear. Older lesions, particularly those containing a mixed bacterial population, may resemble typical abscesses and become encapsulated. Abscesses eventually become sterile and are replaced by fibrous scars. Active lesions may be accompanied by a severe local or diffuse fibrinous peritonitis, or in more chronic cases, by fibrous adhesions to neighbouring structures.
Liver abscesses often occur concurrently with rumenitis (51 per cent of cases), and less often with hyperkeratosis of the forestomachs (14 per cent), abomasal ulcer (10 per cent), and traumatic reticulitis (4 per cent).74
In the rumen, lesions caused by F. necrophorum are generally superficial and consist of focal or diffuse areas of thickened and fused rumen papillae, some of which may demonstrate necrosis or ulceration. Acute lesions (Figure 20), characterized additionally by the presence of oedema, hyperaemia and haemorrhage, may progress to a chronic stage which is typified by loss of papillae, depigmentation and the presence of star-shaped ulcers that heal by granulation and scar tissue formation.
Untoward sequelae of liver abscesses include peritonitis following abscess rupture into the peritoneal cavity, and sudden death from an anaphylactic or toxic reaction where a rupture of an abscess occurs into a hepatic blood vessel. Thrombophlebitis is a possible sequel to hepatic abscessation and arises when a lesion extends into the caudal (posterior) vena cava. This, in turn, can lead to pulmonary thromboembolism (see Pulmonary thromboembolism in cattle, below) endocarditis, multiple lung abscesses or a chronic suppurative pneumonia (i.e. result in the so-called ‘caudal vena cava syndrome’). Thrombosis of the caudal vena cava may also lead to portal hypertension and chronic passive congestion of the liver, resulting in a syndrome of hepatomegaly, ascites and diarrhoea.176
Diagnosis and differential diagnosis
Liver abscesses are rarely diagnosed in live animals. In some animals, the presence of multiple small abscesses in the liver, or even when the abscess is very large, vague signs associated with toxaemia may be evident and a leukocytosis with neutrophilia and increased fibrinogen levels may develop. However, clinical chemistry and liver function tests have not proved to be good indicators of hepatic involvement; they have been found to be of little diagnostic value in predicting the presence of liver abscesses.97 Although ultrasonography may be used as an aid to diagnosis, abscesses in the left half of the liver usually cannot be visualized. Ultrasonography may detect areas of coagulation necrosis within the hepatic parenchyma, if such cases are characterized by a necrotic fluid centre. However, the use of ultrasound for diagnosis of liver abscesses in feedlot cattle is seldom cost-effective.176
Acute clinical cases may be confused with acute peritonitis or traumatic reticuloperitonitis, while chronic cases may be confused with a number of conditions associated with chronic debility and emaciation. Pathologically, rumenitis caused by F. necrophorum must be differentiated from that caused by fungi, usually members of the genera Mucor, Rhizopus and Absidia (see Mycoses). Mycotic rumenitis is a more severe, deeper (often involving the entire thickness of the rumen wall due to infarction) and extensive lesion, and is often fatal.82 A definitive diagnosis of hepatic necrobacillosis rests upon histopathological confirmation or the isolation of F. necrophorum, which may be difficult in cases in which the abscesses are of long duration,55 and selective media may have to be used.
Control
Wherever cattle are raised the control of liver abscesses will be of considerable importance. Losses are associated not only with losses of production and feed efficiency but also with liver condemnation, downgrades at slaughter and other quality parameters.113, 176
The control of liver abscesses in feedlot cattle is based on the use of antimicrobial feed additives and sound nutritional management. The primary control is by preventing, or at least limiting, the occurrence of rumen acidosis through the method of feeding, diet composition, diligent feed bunk management, and the use of buffers in the diet.113 The prevalence of rumenitis and the subsequent development of hepatic abscesses may be reduced by lengthening the transition period (to two to three weeks) from a roughage to a finishing ration, hence gradually adapting cattle to a high-concentrate, low-roughage ration. Increased roughage in the ration will also increase the time of ruminating (chewing) and saliva flow; this will increase the production of buffer to the rumen, thereby reducing rumen acidity. The inclusion of up to 1 per cent calcium carbonate in the diet of cattle in feedlots in order to counteract low pH levels in the rumen may lower the incidence of rumen lesions to negligible levels.
Although the addition of antimicrobial drugs to the diet may detrimentally affect rumen function, the incidence of liver abscesses can be reduced by the continuous feeding, throughout the fattening process, of tylosin at a rate of 100 mg per animal per day (or 10 g per tonne of feed). Virginiamycin at 16 g per tonne, bacitracin, chlortetracycline or oxytetracycline fed continuously at 70 mg per head per day during the finishing period can also be used. Apparently, chlortetracycline has the advantage of having a lesser negative effect on the rumen bacteria. Antimicrobial feed additives also increase average daily weight gain and feed conversion efficiency; however, the ration’s inclusion level for these effects and prevention of liver abscesses is not necessary the same.138 In this overall context, it should be noted that the use of dietary antibiotics in cattle is banned in many countries.
In individual animals, parenteral administration of antimicrobial drugs, such as procaine penicillin and ceftiofur may have a beneficial effect.11 Relapses, however, are quite common following antimicrobial treatment as most drugs are unable to adequately penetrate the liver lesions, thus resulting in incomplete control of the infection.
Clinical trials have demonstrated that vaccination, using a F. necrophorum bacterin, might also have application in decreasing the prevalence of severe liver abscesses at slaughter.

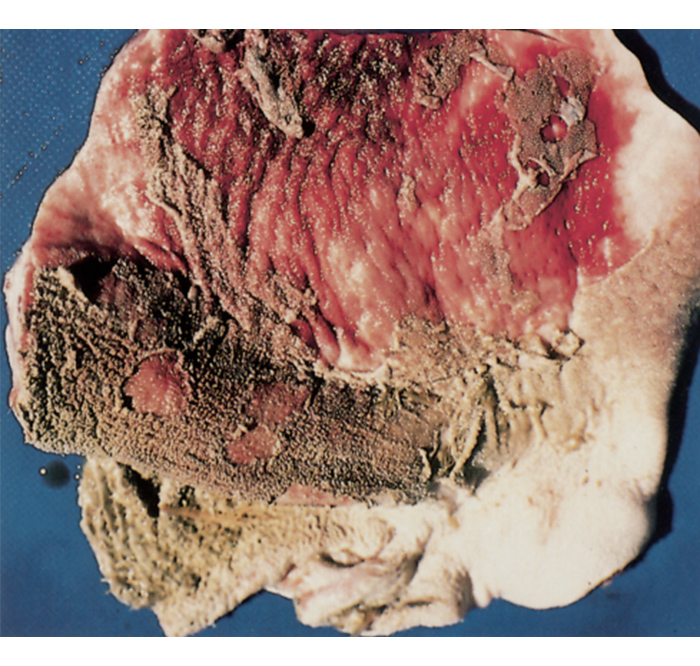
Ovine and caprine hepatic necrobacillosis
Hepatic necrobacillosis occurs sporadically in sheep and goats, but the predisposing factors and portals of entry have not been defined as clearly as in cattle. Necrobacillosis may occur in adults or in lambs and kids; in the former it may be through rumen ulcers, whereas in the latter it may be a consequence of umbilical infection. Lambs and kids kept in wet, intensive and crowded conditions are most commonly affected, in which case the infection usually originates from infected bedding or bedding grounds.
The condition may occur in sheep, Fusobacterium necrophorum may be isolated as the only bacterium involved in up to 45 per cent of cases, or it may be isolated in association with other aerobic and anaerobic bacteria, such as T. pyogenes, Staphylococcus aureus, Pseudomonas aeruginosa, Bacteroides fragilis, Peptostreptococcus anaerobius, Escherichia coli and Clostridium perfringens.193 Abscesses caused by F. necrophorum in sheep livers are similar in appearance and nature to those in cattle, but contrary to the situation in cattle, biovar B is isolated more commonly than biovar A, and often in pure culture.141 Lambs and kids that die of hepatic necrobacillosis are usually in good condition.
Goats affected by hepatic abscesses may develop septicaemia, which in pregnant does may result in abortion.
In young lambs and kids, hepatic necrobacillosis can be controlled by thorough disinfection of the navel at birth and the provision of clean bedding or bedding grounds.
The oral necrobacillosis syndrome
The condition of ‘oral necrobacillosis’ refers to infection of the mucous membranes of the oral cavity, pharynx and larynx of calves with Fusobacterium necrophorum, which can be acute or chronic, and sometimes fatal. A similar disease also occurs in sheep, goats and pigs.
For the general characteristics of F. necrophorum readers should consult the introduction to the section on Anaerobic, Gram-negative, irregular rods.
Within the overall disease syndrome of oral necrobacillosis two separate disease entities are usually recognized: (i) the oral form or necrotic stomatitis, in which lesions are only within the oral cavity; and (ii) the laryngeal form or calf diphtheria, in which lesions are largely confined to the pharynx and the larynx.32
Necrotic stomatitis
Synonym: ulcerative stomatitis
Introduction, aetiology, epidemiology and pathogenesis
Necrotic stomatitis is widely distributed in the world. It usually occurs sporadically, mainly in calves from a few weeks to less than 3 months of age that are housed on straw, rice hulls or woodchips/shavings, although the condition may also be encountered in older cattle. In young calves, the provision of textured calf starter has also been implicated due to the presence of small particulate dry matter, which can become trapped between the gingiva and the erupting molars. However, outbreaks can also occur when calves are housed or closely confined under unhygienic conditions.75 In these cases the infection is probably spread by dirty calfetarias, the teats of calf feeders or by allowing calves to suckle on fingers. Lesions may also follow injury to the buccal cavity caused by oesophageal feeders, which are used to administer colostrum or oral electrolyte solutions, and dosing gun injuries. Necrotic stomatitis may also affect Boer Goat kids grazing on vegetation consisting largely of thorny shrubs and species of grass containing large awns which cause small injuries to the buccal and pharyngeal mucosa.172
When first described in calves in 1876 the disease was considered to be closely related to human diphtheria,35 which is caused by Corynebacterium diphtheriae. In 1884, however, the German bacteriologists Klebs and Löffler proved that it was a distinct disease, and demonstrated that Fusobacterium necrophorum, found invariably along the borders of the lesions, is the leading causing agent of the condition in cattle. Jensen subsequently reported in 1903 that, although the primary lesions usually appear in the mouth, metastatic lesions frequently develop in the lungs, resulting in bronchopneumonia and, in some animals, serofibrinous or purulent pleuritis.
Necrotic stomatitis is caused by infection with F. necrophorum, which is a Gram-negative, non-spore forming, anaerobic bacteria. It is a normal inhabitant of the alimentary tract of animals and humans, and a common inhabitant of the environment of cattle. Fusobacterium necrophorum is likely to contribute to the normal oral flora of the calf. In the normal calf, there are significant mechanical and immunological defence mechanisms that prevent entry of the organism to the tissues of the mouth but, if the calf is debilitated or if the buccal cavity is traumatised, infection can become established. The organism is unable to penetrate healthy, intact mucous membrane or skin, but it readily invades injured tissues to cause extensive necrosis. It is not clear, however, how the organism does establish an infection, because whilst epidemiological factors, such as grossly unhygienic feeding utensils, mucosal abrasion (for example by poor-quality, abrasive, fibrous roughage or very coarse forage or bedding), the eruption of teeth and even vitamin A deficiency are associated with development of the disease, it is difficult to establish the disease experimentally. Hence, it is speculated that other aetiological factors remain to be identified and that F. necrophorum is a secondary, opportunistic invader, rather than the initiating cause of the disease.32 Concurrent disease, such as persistent infection with bovine viral diarrhoea virus, and nutritional deficiency may predispose to such a bacterial infection.
Entry of the causative bacteria results in ulceration of the mucosa of the lips, tongue or cheeks, which occasionally extends to the pharynx. Initial lesions are large, clearly delineated areas of necrosis along the sides of the tongue, on the gums and cheeks (particularly in the region of the fauces of the jaw), palate and pharynx. Lesions in and around the larynx are more typical of ‘oral necrobacillosis’ in older calves (i.e. calf diphtheria) than in young animals. Lesions are dry, yellowish-grey and surrounded by a zone of hyperaemia. There can be progressive sloughing of tissue (and healing by granulation if the animal survives), local spreading of lesions or haematogenous spread resulting in a septicaemia. Death can result from septicaemia, aspiration pneumonia, or from starvation and dehydration.
Clinical signs and pathology
Calves with necrotic stomatitis are initially bright and have a normal temperature, but their breath is foul-smelling with food and saliva dribbling from the mouth. A very characteristic firm swelling on the external cheek is evident; usually only on one side (Figure 21). The size of this swelling is commonly 1.5 to 2 cm in width, which may or may not have a softening at the apex. The animal may show frequent sucking or swallowing movements. When the mouth is closely examined, there is often impaction of food between the molars and the buccal mucosa. Removal of this material will reveal the presence of a characteristic area of necrosis, which is often also present on the edge of the tongue on the same side. Clean lesions are usually well circumscribed with an area of oedema and a necrotic centre. An ulcer may be seen if the necrotic centre has sloughed. The dependent submandibular lymph node is usually enlarged.
As the disease progresses, an elevated temperature (up to 41°C), marked depression and anorexia associated with difficulty in chewing and swallowing may be present. If lesions are present in the tongue or elsewhere in the oral cavity they may seriously interfere with feeding. In some cases, the tongue may be swollen and protrude from the mouth.75 Swelling and inflammation of the tongue and throat region (pharynx) result in a soft cough and progressive dyspnoea. In some cases, exudate from lesions in the upper respiratory tract may be inhaled into the lungs resulting in abscess formation and secondary (broncho)pneumonia.80 There may be a purulent discharge visible at the nares.75 An inspiratory stridor may be audible, suggestive of a partial laryngeal obstruction. There may be rapid loss of weight, due at least in part to the profound anorexia. In a small number of very severe cases death occurs in 2 to 7 days, normally from starvation, toxaemia or secondary pneumonia.

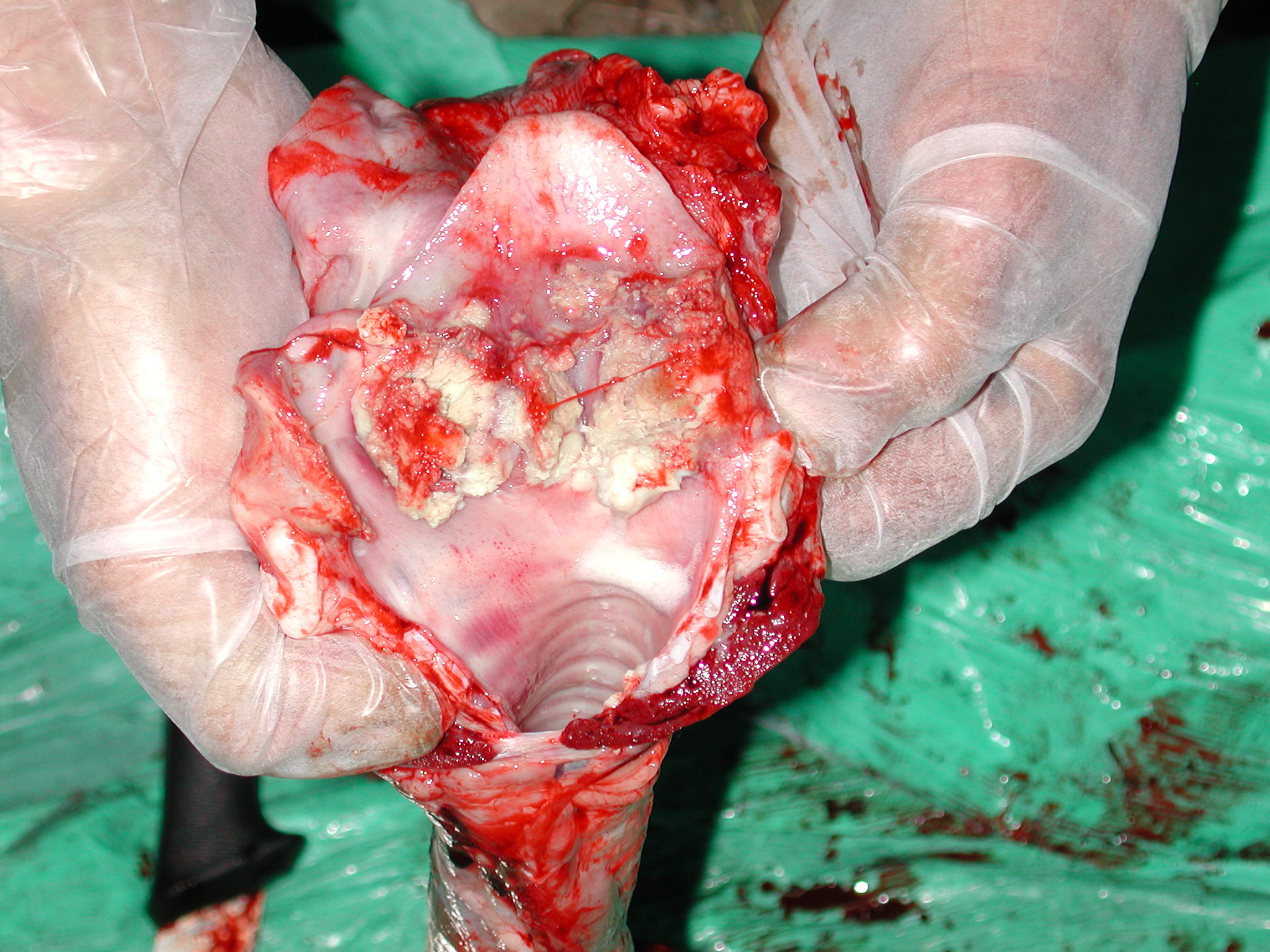
The course of the disease varies from case to case. Some calves may recover spontaneously, but therapy is usually necessary to achieve recovery. Death in untreated calves may occur within four or five days in the more acute disease, or the animal may live for another two to three weeks, eventually dying from starvation, toxaemia or pneumonia.36 In chronic cases, although the appetite may improve to some extent during the course of the disease, body weight is only gained slowly.80
In the outbreaks of necrotic stomatitis in Boer Goat kids that have been recorded in South Africa, the clinical signs and lesions were similar to those seen in calves.172
The initial lesions of ‘oral necrobacillosis’ (necrotic stomatitis and calf diphtheria) consist of one or more irregular, sharply circumscribed, whitish-grey areas of necrosis up to about 50 mm in diameter, which may be surrounded by a marked zone of hyperaemia. The necrotic material is raised slightly above the surrounding normal tissue and is firmly attached to the underlying tissue. As the disease progresses, some or all of it may slough, leaving deep ulcers that heal by granulation.36
Microscopically, the lesions consist of coagulation necrosis of the mucosa and submucosa of affected areas. Colonies of F. necrophorum, as well as other bacteria, are usually visible, particularly at the periphery of the lesions. Highly pleomorphic F. necrophorum organisms, which are filamentous and non-branching, are present in young active lesions, while in chronic lesions the bacteria are coccoid and rod-shaped.
Diagnosis and differential diagnosis
Necrotic stomatitis may be diagnosed on the basis of the clinical signs and observing the characteristic lesions in the oral cavity or pharynx. The diagnosis can be confirmed by isolation of F. necrophorum from swabs of the lesions taken from live animals, or specimens taken aseptically from the affected tissues at necropsy.
Necrotic stomatitis must be differentiated from BVD/mucosal disease, bovine papular stomatitis, mouth injury and foreign bodies. Similar clinical signs may be induced by abscesses caused by Trueperella pyogenes, and acute or chronic pharyngitis caused by trauma that may be caused by dosing procedures, sharp objects in the feed, and, in piglets, erupting teeth or the removal of teeth as a management procedure.
Where oral ulceration exists with high mortality rates, another differential diagnosis called ‘upper alimentary ulcerative syndrome’ also needs to be investigated. This recently identified disease in Victoria, Australia, presents as weight loss and scouring, with upper alimentary tract ulceration and enteritis in weaned calves up to eight months of age.32 A high proportion of affected animals have small ulcers in their mouth or nose. The condition is unresponsive to treatment, including anthelmintic drenches, while sometimes being responsive to antibiotics. Affected calves generally recover over a period of weeks, but may not reach their full potential as adult lactating cows.
On post-mortem examination, severe acute ulcerative glossitis, oesophagitis and pharyngitis with secondary bacterial infection are the most prominent features. Enteritis is seen in some affected calves. Further research is required to determine the risk factors, aetiology and pathophysiology of this emerging disease.
Control
The prognosis for necrotic stomatitis is good with adequate treatment. However, if treatment is delayed, animals can become toxaemic, emaciated and dehydrated, resulting in a much poorer prognosis. Although calves may recover spontaneously, debridement of the necrotic tissue is advisable, if possible, followed by local treatment with povidone iodine solution and parenteral antimicrobial therapy with procaine penicillin at 20 mg/kg. Parenteral oxytetracycline at 10 mg/kg and potentiated sulphonamides (trimethoprim/sulphonamide combination) are also effective. It is advisable to continue the antimicrobial therapy for at least 7 to 10 consecutive days. Affected animals should be isolated and provided with their own designated feeding and drinking equipment.
In the control of necrotic stomatitis, strict attention should be given to the general principles of hygiene. Multiple cases of necrotic stomatitis are usually encountered in calves that are housed in inadequate and unhygienic conditions, have poor feeding hygiene (unwashed utensils, contamination of milk supplies) and/or had inadequate colostrum intake. Hence, if more than a single case occurs, hygiene should be improved, and feeding equipment cleaned and disinfected regularly. The provision of coarse feed that may injure the oral mucous membrane should be avoided.
Calf diphtheria
Synonyms: laryngeal necrobacillosis, necrotic laryngitis
This distinct form of oral necrobacillosis is a disease of young cattle characterized by fever, inspiratory dyspnea and stertorous breathing. It has a worldwide distribution, particularly affecting feedlot cattle between 3 and 18 months of age; however, cases in calves as young as 5 weeks and in cattle as old as 24 months have been documented.
Introduction, aetiology, epidemiology and pathogenesis
Laryngeal necrobacillosis usually occurs sporadically, and is more common in older, weaned calves, although it can occur in younger animals.175 The lesions associated with the condition are largely confined to the larynx and pharynx. The marked inflammatory reaction in the mucosa, submucosa and deeper tissues of the pharynx, larynx and vocal processes of the arytenoid cartilages often causes partial obstruction of the upper respiratory tract. In some animals, lesions may be present in the trachea, nasal passages, oesophagus and forestomachs.
Contact ulceration, the precursor of this condition, is believed to result from frictional contact of both sides of the larynx, most likely initiated by vocalization or paroxysmal coughing, possibly induced by mild respiratory infections or exposure to irritants. Secondary invasion by F. necrophorum produces the more severe lesions of laryngeal necrobacillosis (‘calf diphtheria’). In some animals, papillomavirus infection, rather than F. necrophorum, may invade the contact ulcers.
Swelling and inflammation result in a smaller diameter of the glottis, which may cause severe respiratory distress.
Clinical signs and pathology
Affected animals are typically febrile (up to 41°C), depressed, and show signs of severe Dyspnoea. They extend their head and neck in an effort to breathe, which they do through the mouth. There is stertorous respiration (i.e. strident sound on inspiration) or inspiratory stridor (roaring, honking), audible from a considerable distance; however, frequent harsh coughing is usually not a feature. Affected calves often salivate, are completely anorexic, and have a foul smell on their breath. The laryngeal region is usually swollen and painful, with palpation being resented. Severe cases may die from asphyxiation, with necrotic debris occluding the lumen of the larynx, if animals remain untreated for several days.
The opening of the larynx is usually reddened and narrowed by oedema and inflammation. Well-demarcated, yellow areas of necrosis surrounded by a zone of hyperaemia may be observed on one or both arytenoid cartilages (Figure 22).
Diagnosis and differential diagnoses
Diagnosis of laryngeal necrobacillosis is based on the inspiratory dyspnoea and stridor, fever and visualization of the lesion. The pharynx and larynx may be visualized using a cylindrical speculum positioned over the tongue and a bright light source to illuminate the area involved.
The condition must be differentiated from foreign bodies, pharyngeal abscess or traumatic injuries to the pharynx or larynx (e.g. drenching or inexpert attempts at passing a stomach tube).
Management
The prognosis is usually good if the condition is detected very early and aggressive treatment implemented. However, if treatment is delayed, extensive necrosis of the laryngeal cartilage (suppurative chondritis) may occur, with subsequent damage to the laryngeal architecture. These animals do not respond well to treatment, and continue to show signs of ill-thrift and dyspnoea.
In the laryngeal form of ‘oral necrobacillosis’, parenteral antibiotic (procaine penicillin or broad-spectrum antibiotics, such as potentiated sulphonamides and oxytetracycline) therapy needs to be continued for an extended period (i.e. 2 to 3 weeks). Narrowing of the airway contributes to turbulent airflow, which exacerbates inflammation of the mucosa and narrowing of the airway. Providing shade for affected calves during hot weather is important to mitigate exacerbation of the respiratory distress induced by panting. Corticosteroids, rather than non-steroidal anti-inflammatory drugs, are indicated during the acute stage to reduce laryngeal oedema and assist breathing.145, 175
If breathing is extremely laboured, it may be necessary to perform a tracheotomy and insert a tracheal tube. The instantaneous relief provided by tracheostomy and the advantages of diminished laryngeal and pharyngeal movements during respiration can be considerable.
Laryngotomy and surgical removal of necrotic tissue may be an option for valuable calves that are refractory to medical therapy.
Because laryngeal necrobacillosis occurs sporadically, often in well-grown beef calves, without obvious cause, there are no specific control measures, although an association with grazing paddocks containing gorse has been suggested.145
Other conditions caused by Fusobacterium necrophorum, Bacteroides spp. and members of related genera
Pulmonary thromboembolism in cattle
Pulmonary thromboembolism in cattle is one of the possible complications associated with hepatic abscessation caused by Fusobacterium necrophorum and other bacteria species. (see Bovine hepatic necrobacillosis, above). It is an uncommon, sporadic, but invariably fatal condition, and occurs as a sequel to the development of septic thrombophlebitis of the caudal vena cava or one of the larger branches of a hepatic vein, with consequent involvement of the caudal vena cava. Death is ultimately due to the subsequent rupture of a pulmonary arterial aneurysm(s).
Hepatic thrombophlebitis arises most commonly by direct extension of an inflammatory process of a hepatic abscess located in close proximity to the blood vessel concerned, but it may similarly arise as a result of an abscess lying outside the liver, but adjacent to the caudal vena cava, such as one situated between the liver and the diaphragm.146 Selman and his colleagues reviewed the clinical and pathological aspects of 12 cases of thromboembolism in cattle.146 The thrombi which develop in the caudal vena cava may extend from the liver to the right atrium of the heart and may totally or partially occlude the vessel, resulting in chronic passive venous congestion of the liver. Septic emboli dislodged from the thrombus in the vena cava spread to the lungs, where the principle lesions to develop are multiple pulmonary abscesses, suppurative pneumonia, and erosion of pulmonary arterial walls with intrapulmonary haemorrhage. Haemoptysis and bilateral epistaxis of arterial blood is almost pathognomonic for this disease and will prove to be fatal. An endocarditis may be present in a small percentage of animals.177
The history of the disease in affected animals varies from that of a ‘sudden death’ syndrome to one of a respiratory disease with a short-term response to antibiotic therapy, but with signs of shallow painful respirations and coughing re-appearing 3 to 10 days later. The course of the disease usually varies in length from a few to more than 100 days. One or several of the following clinical signs may be shown:146 loss of weight, fever (not constant), tachypnoea, hyperpnoea, dyspnoea, widespread crackles and wheezes on auscultation, coughing, thoracic pain, tachycardia, evidence of cardiac failure, hepatomegaly, anaemic mucous membranes (as a result of pneumorrhagia), haemoptysis, bilateral epistaxis, and melaena (the result of swallowing blood from the lungs). The four most constant presenting signs that are of diagnostic value appear to be anaemia, bilateral epistaxis, haemoptysis and widespread crackles and wheezes on auscultation of the lungs, while thoracic pain and hepatomegaly are also commonly encountered.146 Bilateral epistaxis is the cardinal clinical sign of advanced disease and indicates a hopeless prognosis. Death usually happens soon after massive intrabronchial haemorrhage has occurred, but is often preceded by respiratory signs of at least several days duration.146
Diagnosis of pulmonary thromboembolism is difficult until the characteristic haemoptysis and bilateral epistaxis occurs. Prior to that there may be recurrent pyrexia with vague respiratory signs and weight loss. Although ultrasonographic detection of the thrombus in the caudal vena cava can be undertaken,28 such examination is highly unlikely to happen in a clinical practice setting.
There is no effective treatment in cattle with significant pulmonary haemorrhage. Control of the disease relies on steps taken to control the rumenitis-hepatic abscess complex.175 This in turn relies largely on controlling rumen acidosis.
Necrotic rhinitis of pigs
Synonym: Bull nose
Necrotic rhinitis or bull nose is often confused with atrophic rhinitis. It is an uncommon, sporadic disease of young, growing pigs and may occur in herds where atrophic rhinitis is present, sometimes even in the same animal. However, there appears to be no association between the two conditions. Necrotic rhinitis lesions develop as a localized necrotic cellulitis of the soft tissues of the snout and face, but may spread to involve bone. Severe, irregular, asymmetrical swelling and deformity of the snout and face occurs as a result of localized necrosis, suppuration and connective tissue proliferation. The common existence of Fusobacterium necrophorum bacteria in the lesions implies that any injury to the face, or nasal or oral cavities, may lead to invasion, particularly if the environmental conditions are dirty and severely contaminated. In some cases, spirochaetes (see Borrelia suilla infection) and other bacteria species may also be involved. Over the last 2 to 3 decades the incidence of necrotic rhinitis has progressively diminished, probably due to improved hygiene in piggeries.
Bacteria may gain entry through injuries, often being inconspicuous, to the oral and nasal mucosa or face. Bite wounds may also play a role in the pathogenesis. A common portal of entry of organisms in piglets is injury to the gums that may arise if the needle teeth (wolf teeth or the deciduous third incisors) are clipped too short,147 then spread to bony tissue with a resultant osteitis occurring via the gingival lymphatics.82
The prevalence of necrotic rhinitis in herds is generally low, only one or two pigs being affected.147 In affected animals, local swelling is obvious and extensive lesions may interfere with respiration and mastication. Any partial obstruction of the upper respiratory tract will be accompanied by snuffling and sneezing. A foul-smelling nasal discharge and occasional epistaxis are also common features of the disease.147 Toxaemia combined with inappetence and difficulties with mastication may lead to significant weight loss and some deaths. Some animals may show a purulent ocular discharge.147
The localized swelling is usually hard, and when incised will reveal a mass of greyish, foul-smelling, necrotic tissue with massive connective tissue proliferation.139, 147 Soft tissues, facial bones and sinuses are usually involved in the inflammatory process. However, the skin remains usually intact.
Necrotic rhinitis should be differentiated from progressive atrophic rhinitis (see Progressive atrophic rhinitis) and necrotic ulcer. Pigs suffering from progressive atrophic rhinitis often show marked deviation of the snout, but no swelling of the region.147 Also, oral and facial lesions are characteristic features of necrotic rhinitis, not so of atrophic rhinitis. Necrotic ulcer in pigs may also involve the mouth and face; however, the lesions are of an erosive nature rather than being necrotic.
The treatment of early cases is by surgical intervention and the topical application of antimicrobial drugs, such as sulphonamides or tincture of iodine.147 The oral administration of sulphamethazine (sulphadimidine) has proved successful in young pigs.50 Treatment with other antimicrobial drugs to which F. necrophorum is susceptible would probably provide a similar result in controlling the infection if applied in the early stages of the disease. It is doubtful if treatment of advanced cases is advisable.147 Control and prevention in piggeries involves improvement of sanitation, elimination of injuries and disinfection of pens. In herds where the disease occurs repeatedly, great care should be taken in the clipping of needle teeth.147
Foot rot in pigs
Synonym: bush foot
Foot rot in pigs has been reported from numerous countries and is probably universal in occurrence. The condition is similar clinically to foot rot in other species, although the cause of the disease seems to be different; in most instances it is akin to foot abscess in sheep. In pigs the term ‘foot rot’ is used to describe the disease that follows when a traumatic lesion in the claw of a pig of any age becomes secondarily invaded by infectious agents.161 The most common claw lesions which are involved are sand cracks (including false sand cracks) in the claw wall; heel, toe and sole erosions; lesions of the white line and heel flaps.124 Bruising of the heel/sole junction may precede the development of erosive lesions.192 Once an infection has gained entry into a claw it may spread to the deeper tissues and neighbouring structures, such as tendons, joints, ligaments and bone. Although all claws may be affected, lesions appear to be most common in the abaxial (lateral) claw of the hind feet.124
Common organisms which have been isolated from affected feet comprise Fusobacterium necrophorum, Trueperella (formerly Arcanobacter) pyogenes, staphylococci and spirochaetes. In addition, Dichelobacter (formerly Bacteroides) nodosus and other anaerobic bacteria, including Prevotella, Peptostreptococcus, Porphyromomonas, Bacteroides and Eubaterium, have all been isolated from affected feet in an outbreak of foot rot on a semi-extensive pig farm in Spain.126 The infection may be introduced into a piggery by the introduction of infected pigs. Once established, foot rot may then spread rapidly to become a herd problem.
Factors that predispose to traumatic foot lesions are the abrasive quality of rough concrete pen floors, the chemical effects of newly poured alkaline concrete, and poor bedding. By themselves the resulting lesions do not normally cause lameness, except when they are extensive; however, when pigs are also reared in damp, unhygienic conditions infection and subsequent lameness may follow.124, 161, 192 Wet conditions underfoot may cause maceration of the claw horn, thereby exacerbating any abrasive effect of the flooring. Foot abscess in piglets is usually associated with the animals being reared on woven wire floors.60 Dietary deficiencies, particularly biotin deficiency may also result in foot lesions that predispose to secondary infection. A high incidence of infection and clinical lameness may arise in herds where the adverse predisposing causes prevail.
In cases where claw lesions are extensive or where infection has occurred marked lameness will be apparent. Usually only the lateral hind claw of one foot will be affected. The affected claw is usually swollen, warm and painful. The degree of lameness depends on the extent of the lesions. Severe lameness is manifested when sinus tracts and abscesses break out at the coronet, leading to the development of discharging granulomatous lesions. Usually, there is only a minimal amount of purulent material present. If significant swelling occurs due to cellulitis it often extends higher up the limb to reach the hock or carpus.161 Pain and lameness may lead to significant production losses. Furthermore, lameness in sows may cause clumsiness and bad mothering, whereas in boars it may lead to infertility, due to the inability to mate.121, 124 Secondary abscessation in other parts of the body is an occasional sequel of foot rot and may result in partial or total condemnation of the carcass at slaughter.
Foot abscesses in neonatal pigs are characterized by necrotic pododermatitis, severe osteomyelitis, arthritis and tendosynovitis.61 The primary locations of injury are situated at either the point of the toe at the white line, the bulb of the heel or the haired skin around the coronet, including the interdigital area. About 6 per cent of piglets may develop foot abscess prior to weaning, with approximately one-third of litters being affected.
Bacteriological examination of discharge from the lesions may assist in deciding the treatment to be implemented. The rational treatment of individual cases includes cleaning and surgical paring of claw lesions, combined with topical and/or parenteral administration of antimicrobial drugs such as penicillin or broad-spectrum antibiotics. In cases of deeply infected feet the recovery rate will be only fair at best with treatment. Exposing pigs to a footbath containing a 5 to 10 per cent solution of formalin or copper sulphate two or three times per week may reduce the prevalence of foot rot.192
To control foot rot, possible predisposing causes should be prevented. Preventing excessive wear of the claws by the use of adequate bedding and less abrasive flooring in pig pens is a logical control measure. In addition, any existing dietary deficiency should be corrected, especially with regards to biotin, as it has been found that biotin supplementation of the diet of pigs resulted in fewer and less severe foot lesions.123
Cara inchada
Cara inchada (Portugese for ‘swollen or enlarged face’) is a rapidly progressive periodontal disease that occurs during the time of tooth eruption of young cattle mainly between the ages of 2 and 14 months. It occurs in animals grazing new pastures sown in ground of recently cleared forest areas of central-western Brazil, where in some districts it constitutes a serious economic problem.25 In some herds the prevalence rate may exceed 50 per cent. Clinically it is characterized by a unilateral or bilateral bulging of the part of the face over the lesion in the maxilla or mandible.
The precise aetiology and pathogenesis of cara inchada is still uncertain; however, Prevotella melaninogenica (formerly Bacteroides melaninogenicus) and Trueperella (formerly Arcanobacter) pyogenes have been isolated from the periodontal lesions. The condition appears to be associated with the altered ecological soil conditions that follow the clearing of forests or ‘cerrado’ (savanna) and the establishment of cultivated pastures of grasses, such as Panicum maximum (buffalograss) and Brachiaria decumbens (signal grass) for cattle grazing.22, 25, 40 The bacteria species associated with the disease possess enough pathogenic potential, through the production of enzymes and endotoxins, to cause primary destruction of the periodontal tissues.40 There is strong evidence that an augmented concentration of antibiotics, such as streptomycin and actinomycin, produced by increased numbers of actinomycetes, including those of the genus Streptomyces, that are present in the disturbed virgin soils, could be the determining factor for the development of the rapidly progressive periodontitis when ingested with the forage. There is experimental evidence that this factor is also present in the milk of cows with cara inchada-diseased calves. In vitro assays have shown that P. melaninogenica organisms treated with sub-inhibitory concentrations of such antibiotics were ten times more likely to adhere to the bovine gingival and sulcus epithelial cells than were untreated bacteria. It is thought that such enhanced adherence of the bacteria present in the subgingival space induces an increased degree of pathogenicity in them.63, 92 Prevotella melaninogenica can be isolated, although in small numbers, from the gums of healthy calves.63 Although not proven, trace mineral deficiencies are assumed to predispose to the disease.128
Cara inchada is a progressive purulent periodontitis and secondary ossifying periostitis of the tooth cavity of one or more of the premolar or molar teeth, mainly of the upper jaw, which leads to localized bone resorption with cavitation, proliferation of bone, and loosening and eventual loss of the tooth or teeth involved. In at-risk areas, attack rates and case fatality rates are often high, mainly due to malnutrition and emaciation. The frequent diarrhoea observed in calves affected by cara inchada is suggested to occur due to changes in the microflora of the digestive tract.40
Removal of diseased cattle from a herd reduces the prevalence of the condition.24 The decline in prevalence and eventual disappearance of the disease from affected herds within a few years can possibly be explained by the establishment of an equilibrium in the soil microflora during this period of time,40 although renewed outbreaks of the disease have occurred in former cara inchada-prone areas following fresh cultivation of the soil after many years. The bacterial species which have been isolated from the lesions are susceptible in vivo to penicillin, tetracycline, virginiamycin and erythromycin.25 The inclusion of spiramycin or virginiamycin in mineral licks or the mineral mix fed to the cattle will prevent the disease.
Other Bacteroides spp. infections
Bacteroides spp. are associated with different non-specific disease conditions in livestock.18, 19, 22, 111, 158 For example, Prevotella melaninogenica (formerly Bacteroides melaninogenicus) has been isolated from cattle suffering from interdigital necrobacillosis (foot rot), traumatic pericarditis and peritonitis, suppurative arthritis and fibrinous pneumonia; from sheep with fibrinous pneumonia, polyarthritis, purulent rhinitis, septicaemic pasteurellosis and suppurative meningitis; from horses affected by pleuropneumonia and deep draining wounds; and from pigs with preputial ulceration, pneumonia and enteritis. Bacteroides fragilis has been isolated from calves, lambs and foals with diarrhoea; from horses with pleuropneumonia and deep draining wounds; and from pigs with preputial ulceration.
Bacteria species other than P. melaninogenica and B. fragilis that have been associated with equine pleuropneumonia are B. oralis, B. asaccharolyticus, B. splanchnicus, B. uniformis, B. thetaiotaomicron, B. ruminicola and an unnamed species.158 Unnamed species have also been isolated from septic arthritis in horses103 and from a cerebral abscess in a heifer.104
The relatively high prevalence of Bacteroides spp. infections in pleuropneumonic lesions in horses indicates that specimens for both anaerobic and aerobic culture should be submitted from every horse with pleural effusion, irrespective of whether or not the specimen has a putrid odour.158 The breath of such animals may also have a similar unpleasant odour.
Antimicrobial therapy of Bacteroides spp. infections should always be based on the result of an antibiogram (i.e., an overall profile of antimicrobial susceptibility testing results of a specific micro-organism to a series of antimicrobial drugs),19 as well as on the nature and sensitivity of the other species of bacteria with which the organism is usually associated in the lesions. The results of aerobic cultures may dictate that a combination of drugs will be required. In human medicine, metronidazole, chloramphenicol and clindamycin are routinely used against B. fragilis infections.19 Penicillin, however, is the drug of choice if the anaerobe organism is not B. fragilis.19
Prevotella melaninogenica, Fusobacterium necrophorum, Trueperella (formerly Arcanobacter) pyogenes, Peptostreptococcus indolicus, and Streptococcus dysgalactiae are among the many factors that have been implicated in the complex aetiology of summer mastitis, which occurs in outbreaks in cattle during the summer months in Europe and Scandinavia.102 Sporadic cases of summer mastitis have also been reported from New Zealand and Australia.
References
- AALBAK, B., 1971. Sphaerophorus necrophorus. A study of 23 strains. Acta Veterinaria Scandinavica, 12, 344-364.
- ALLWORTH, B., 1990. Foot rot — control and eradication. In: Sheep Medicine, Proceedings of the Sandy and Georgina Reid Memorial Refresher Course for Veterinarians, 16–20 July 1990, University of Sydney, Australia.
- ALLWORTH, M. B., 1995. Investigations of the eradication of foot rot. Ph.D. Thesis, University of Sydney, Australia.
- ALLWORTH, M. B. & EGERTON, J. R., 2018a. Comparison of footbathing and vaccination to control ovine footrot in an experimentally infected flock. Australian Veterinary Journal, 96, 395-399.
- ALLWORTH, M. B. & EGERTON, J. R., 2018b. Relationship between the likelihood of footrot elimination from a flock and the virulence of the strain of Dichelobacter nodosus present. Australian Veterinary Journal, 96, 400-407.
- AMSTUTZ, H. E., 1985. Prevention and control of lameness in dairy cattle. Veterinary Clinics of North America, 1, 25-37.
- ARKINS, S., 1981. Lameness in dairy cows. Irish Veterinary Journal, 35, 135-140.
- ARKINS, S., 1981. Lameness in dairy cows. Irish Veterinary Journal, 35, 163-170.
- ARKINS, S., 1982. Lameness: An often neglected factor in dairy cow health. Farm and Food Research, 13, 90.
- ATKINS, J. W., 1986. The use of a zinc sulphate formulation for the eradication of foot rot during a period favouring spread of the disease. In: STEWART, D. J., PETERSON, J. E., MCKERN, N. M. & EMERY, D. L., (eds.). Foot rot in Ruminants, Proceedings of a Workshop, Melbourne 1985, CSIRO Division of Animal Health, Australian Wool Corporation, Australia.
- BABA, E., FUKATA, T., ARAKAWA, A., IKAWA, H. & TAKEDA, M., 1989. Antibiotic susceptibility of Fusobacterium necrophorum from bovine hepatic abscesses. British Veterinary Journal, 145, 195-197.
- BAGGOTT, E., 1982. Hoof lameness in dairy cattle. In Practice (a supplement to The Veterinary Record), September, 133-141.
- BARBER, D. M. L., 1979. Foot rot in sheep. Veterinary Record, 104, 194-195.
- BATH, G. & BISHOP, G., 1984. Allerton Regional Veterinary Laboratory, Private Bag X2, Cascades 3202, South Africa. Unpublished data.
- BERG, J. N. & LOAN, R. W., 1975. Fusobacterium necrophorum and Bacteroides melaninogenicus as etiologic agents of foot rot in cattle. American Journal of Veterinary Research, 36, 1115-1122.
- BERG, J. N., MAAS, J. P., PATERSON, J. A., KRAUSE, G. F. & DAVIS, L. E., 1984. Efficacy of ethylenediamine dihydriodide as an agent to prevent experimentally induced bovine foot rot. American Journal of Veterinary Research, 45, 1073-1078.
- BERG, J. N. & SCANLAN, C. M., 1982. Studies of Fusobacterium necrophorum from bovine hepatic abscesses: Biotypes, quantitation, virulence, and antibiotic susceptibility. American Journal of Veterinary Research, 43, 1580-1586.
- BERKHOFF, G. A., 1977. Recovery and identification of anaerobes in veterinary medicine: A two-year experience. Veterinary Microbiology, 2, 237-252.
- BERNARD-STROTHER, S. & MANSMANN, R. A., 1985. Diagnosis and treatment of anaerobic bacterial pleuropneumonia in six horses. The Compendium on Continuing Education for the Practising Veterinarian, 7, S341-S349.
- BERRY, S. L., READ, D. H., FAMULA, T. R., MONGINI, A. & DOPFER, D., 2012. Long‐term observations on the dynamics of bovine digital dermatitis lesions on a California dairy after topical treatment with lincomycin HCl. Veterinary Journal, 193, 654-658.
- BEVERIDGE, W. I. B., 1941. Foot rot in sheep: A transmissible disease due to infection with Fusiformis nodosus (n. sp.). Studies on its cause, epidemiology and control. Bulletin of the Council for Scientific and Industrial Research of Australia, 140, 1-53.
- BIBERSTEIN, E. L., KNIGHT, H. D. & ENGLAND, K., 1968. Bacteroides melaninogenicus in diseases of domestic animals. Journal of the American Veterinary Medical Association, 153, 1045-1049.
- BICALHO, R. C., MACHADO, V. S. & CAIXETA, L. S., 2009. Lameness in dairy cattle: a debilitating disease or a disease of debilitated cattle? Journal of Dairy Science, 92, 3175-3184.
- BLOBEL, H., DÖBEREINER, G., ROSA, I. V., LIMA, F. G. F. & DOS SANTOS DURA, I., 1987. Bacterial investigations of a periodontal disease — cara inchada — in Brazilian cattle. Tierärztliche Umschau, 42, 152-157.
- BLOBEL, H., DÖBEREINER, J., LIMA, F. G. F. & ROSA, I. V., 1984. Bacterial isolations from ‘cara inchada’-like lesions of cattle. Pesquisa Veterinária Brasileira, 4, 73-77.
- BLOWEY, R. W., 1998. Necrotic heel track — is this a sole ulcer at a caudal site? The 10th International Symposium on Lameness in Ruminants, Lucerne, Switzerland, 132-133.
- BLOWLEY, R. W., DONE, S. H. & COOLEY, W., 1994. Observations on the pathogenesis of digital dermatitis in cattle. Veterinary Record, 135, 115-117.
- BRAUN, U., FLÜCKIGER, M., FEIGE, K. & POSPISCHIL, A., 2002. Diagnosis by ultrasonography of congestion of the caudal vena cava secondary to thrombosis in 12 cows. Veterinary Record, 150, 209-213.
- CASEY, R. H. & MARTIN, P. A. J., 1988. Effect of foot paring of sheep affected with foot rot on response to zinc sulphate/sodium lauryl sulphate foot bathing treatment. Australian Veterinary Journal, 65, 258-259.
- CHESTERTON, R. N., LAWRENCE, K. & LAVEN, R. A., 2008. A descriptive analysis of the foot lesions identified during veterinary treatment for lameness on dairy farms in north Taranaki. New Zealand Veterinary Journal, 56, 130-138.
- CHOQUETTE-LEVY, L., BARIL, J., LEVY, M. & ST-PIERRE, H., 1985. A study of foot disease of dairy cattle in Quebec. Canadian Veterinary Journal, 26, 278-281.
- CHUCK, G. M., PARKINSON, T. J. & VERMUNT, J. J., 2019. Calves: management and diseases. In: PARKINSON, T. J., VERMUNT, J. J., MALMO, J. & LAVEN, R. A., (eds.). Diseases of Cattle in Australasia, 2nd edition, Auckland, New Zealand: Massey University Press.
- CLARK, B. L., EMERY, D. L. & STEWART, D. J., 1986. In: STEWART, D. J., PETERSON, J. E., MCKERN, N. M. & EMERY, D .L., (eds.). The aetiology and prevention of interdigital necrobacillosis (foot abscess) in cattle. Proceedings of a Workshop, Melbourne, 1985. CSIRO Division of Animal Health, Australia, Wool Corporation, Australia.
- COOK, N. B. & CUTLER, K. L., 1995. Treatment and outcome of a severe form of foul-in-the-foot. Veterinary Record, 136, 19-20.
- DAMMANN, C., 1876. Die Diphtherie der Kalber eine neue, auf den Menschen übertragbare Zoonose. Deutsch Zeitschrift für Tiermedicin und Vergleichende Pathologie, 3, 1-27.
- DAVIES, G. O., 1947. Gaiger and Davies’ Veterinary Pathology and Bacteriology. 3rd edn. London: Baillière, Tindall & Cox.
- DEMERTZIS, P. N. & MILLS, C. F., 1973. Oral zinc therapy in the control of infectious pododermatitis in young bulls. Veterinary Record, 93, 219-222.
- DHUNGYEL, O., HUNTER, J. & WHITTINGTON, R., 2014. Footrot vaccines and vaccination. Vaccine, 32(26), 3139-3146.
- DHUNGYEL, O., SCHILLER, N., EPPLESTON, J., LEHMANN, D., NILON, P., EWERS, A. & WHITTINGTON, R., 2013. Outbreak-specific monovalent/bivalent vaccination to control and eradicate virulent ovine footrot. Vaccine, 31(13), 1701-1706.
- DÖBEREINER, J., 1990. Zur Ätiologie der ‘Cara inchada’, einer paradontalen Erkrankung der Jungrinder in Brasilien. Deutsche Tierärztliche Wochenschrift, 97, 482-490.
- DOUGHERTY, R. W., RILEY, J. L., BAETZ, A. L., COOK, H. M. & COBURN, K. S., 1975. Physiologic studies of experimentally grain-engorged cattle and sheep. American Journal of Veterinary Research, 36, 833-835.
- EDWARDS, B., 1980. Foot lameness in cattle. In Practice, 2, 25-31.
- EDWARDS, G. B., 1972. Foot lameness in cattle. Veterinary Annual, 7-14
- EGERTON, J. R., 1986. Control and eradication of ovine foot rot. In: STEWART, D. J., PETERSON, J. E., MCKERN, N. M. & EMERY, D. L., (eds.). Foot rot in Ruminants, Proceedings of a Workshop, Melbourne, 1985, CSIRO Division of Animal Health, Australian Wool Corporation, Australia.
- EGERTON, J. R., GHIMIRE, S. C., DHUNGYEL, O. P., SHRESTHA, H. K., JOSHI, H. D., JOSHI, B. R., ABBOTT, K. A. & KRISTO, C., 2002. Eradication of virulent footrot from sheep and goats in an endemic area of Nepal and an evaluation of specific vaccination. Veterinary Record, 151(10), 290-295.
- EGERTON, J. R., LAING, E. A. & MULLEY, R. C., 1985. Failure of oral zinc therapy to alleviate Bacteroides nodosus infections in cattle and sheep. Australian Veterinary Journal, 62, 85.
- EGERTON, J. R., PARSONSON, I. M. & GRAHAM, N. P. H., 1968. Parenteral chemotherapy of ovine foot rot. Australian Veterinary Journal, 44, 275-283.
- EGERTON, J. R., ROBERTS, D. S., GRAHAM, N. P. H. & PARSONSON, I. M., 1966. Ovine interdigital dermatitis and its relationship to foot rot and foot abscess. Australian Veterinary Journal, 42, 440.
- EGERTON, J. R., ROBERTS, D. S. & PARSONSON, I. M., 1969. The aetiology and pathogenesis of ovine foot rot. I. A histological study of the bacterial invasion. Journal of Comparative Pathology, 79, 207-216.
- EIELAND, E. & FAANES, T., 1950. Actinomyces necrophorum infection in suckling pigs and experiment on treatment with sulphamethazine. Nordisk Veterinaermedicin, 2, 204-208.
- EMERY, D. L., 1987. Immunity against anaerobic bacterial infections. Veterinary Immunology and Immunopathology, 15, 1-57.
- EMERY, D. L., STEWART, D. J. & CLARK, B. L., 1984. The comparative susceptibility of five breeds of sheep to foot rot. Australian Veterinary Journal, 61, 85-88.
- EMERY, D. L., VAUGHAN, J. A., CLARK, B. L., DUFFY, J. H. & STEWART, D. J., 1985. Cultural characteristics and virulence of strains of Fusobacterium necrophorum isolated from the feet of cattle and sheep. Australian Veterinary Journal, 62, 43-46.
- EVANS, N. J., BLOWEY, R. W., TIMOFTE, D., ISHERWOOD, D. R., BROWN, J. M., MURRAY, R., PATON, R. J. & CARTER, S. D., 2011. Association between bovine digital dermatitis treponemes and a range of 'non-healing' bovine hoof disorders. Veterinary Record 168, 214-217.
- FALES, W. H. & TERESA, G. W., 1972. A selective medium for the isolation of Sphaerophorus necrophorus. American Journal of Veterinary Research, 33, 2317-2321.
- FALES, W. H., WARNER, J. F. & TERESA, G. W., 1977. Effects of Fusobacterium necrophorum leukotoxin on rabbit peritoneal macrophages in vitro. American Journal of Veterinary Research, 38, 491-495
- FREDERICK, L. D., 1943. The economic and nutritional importance of bovine hepatic disturbances. Journal of the American Veterinary Medical Association, 102, 338-345.
- FRISCH, J. E., 1976. The comparative incidence of foot rot in Bos taurus and Bos indicus cattle. Australian Veterinary Journal, 52, 228-229.
- GARCIA, M. M., NEIL, D. H. & MCKAY, K. A., 1971. Application of immunofluorescence to studies on the ecology of Sphaerophorus necrophorus. Applied Microbiology, 21, 809-814.
- GARDNER, I. A. & HIRD, D. W., 1994. Risk factors for development of foot abscess in neonatal pigs. Journal of the American Veterinary Medical Association, 204, 1062-1067.
- GARDNER, I. A., W., H. D., M., S. N. & PIERCE, R. J., 1990. Clinical, pathologic, and microbiologic findings of foot abscess in neonatal pigs. Journal of the American Veterinary Medical Association, 196, 1791-1794.
- GRAHAM, N. P. H. & EGERTON, J. R., 1968. Pathogenesis of ovine foot-rot: the role of some environmental factors. Australian Veterinary Journal, 44, 235-240.
- GRASSMAN, B., DÖBEREINER, J., DUTRA, I. S., KOPP, P. A. & BLOBEL, H., 1997. Adherence and experimental infection of bacteria associated with periodontal infections of young cattle in Brazil (‘cara inchada’). Pesquisa Veterinária Brasileira, 17, 123-125.
- GREENOUGH, P. R., 1980. The conformation of cattle. Bovine Practice, 1, 20-34.
- GREENOUGH, P. R., 1987. An illustrated compendium of bovine lameness. Part 1: Modern Veterinary Practice, January, 6-9.
- GREENOUGH, P. R., 1987. An illustrated compendium of bovine lameness. Part 4: Modern Veterinary Practice, January, 6–9.
- GREENOUGH, P. R., 1990. Observations on bovine laminitis. In Practice, 12, 169-173.
- GREENOUGH, P. R. & VERMUNT, J. J., 1991. Evaluation of subclinical laminitis in a dairy herd and observations on associated nutritional and management factors. Veterinary Record, 128, 11-17.
- GREENOUGH, P. R., VERMUNT, J. J., MCKINNON, J. J., FATHY, F. A., BERG, P. A. & COHEN, R. D. H., 1990. Laminitis-like changes in the claws of feedlot cattle. Canadian Veterinary Journal, 31, 202-208.
- GREENOUGH, P. R. & WEAVER, A. D., 1997. Lameness in Cattle. 3rd edn. Philadelphia: W.B. Saunders Company.
- GREGORY, T. S., 1939. Foot-rot in sheep. Australian Veterinary Journal, 15, 160-167.
- GURUNG, R. B., DHUNGYEL, O. P., TSHERING, P. & EGERTON, J. R., 2006. The use of an autogenous Dichelobacter nodosus vaccine to eliminate clinical signs of virulent footrot in a sheep flock in Bhutan. Veterinary Journal, 172(2), 356-363.
- HALE, W. H., 1985. Liver abscess and founder in feedlot cattle. Animal Health and Nutrition for Feed Animal Veterinarians, 40, 12-20.
- HAN, I. K., SEO, B. K., CHANG, K. J. & YOON, H. J., 1985. Abattoir survey of liver abscesses in cattle in Korea. Korean Journal of Veterinary Public Health, 9, 17-24.
- HENNING, M. W., 1962. The Calf in Health and Disease. Johannesburg: Central News Agency, Ltd.
- HINTON, D. G., 1991. Eradication of actively spreading ovine foot rot. Australian Veterinary Journal, 68, 118-119.
- HULL, B. L., 1993. Diseases of the musculoskeletal system. In: HOWARD, J. L., (ed.). Current Veterinary Therapy 3: Food Animal Practice. Philadelphia: W.B. Saunders Company
- JENSEN, R., CONNEL, W. E. & DEEM, A. W., 1954. Rumenitis and its relation to rate of change of ration and the proportion of concentrate in the ration of cattle. American Journal of Veterinary Research, 15, 425-428.
- JENSEN, R., DEANE, H. M., COOPER, L. J., MILLER, V. A. & GRAHAM, W. R., 1954. The rumenitis-liver abscess complex in beef cattle. American Journal of Veterinary Research, 15, 202-216.
- JENSEN, R. & MACKEY, D. R., 1971. Diseases of Feedlot Cattle. Philadelphia: Lea & Febiger.
- JOHNSON, D. W., DOMMER, A. R. & KIGER, D. G., 1969. Clinical investigations of infectious foot rot of cattle. Journal of the American Veterinary Medical Association, 155, 1886-1891.
- JUBB, K. V. F., KENNEDY, P. C. & PALMER, N., 1985. Pathology of Domestic Animals. 3rd edn. San Diego: Academic Press Inc.
- KANOE, M., 1990. Fusobacterium necrophorum haemolysin in bovine hepatic abscess. Journal of Veterinary Medicine, Series B, 37, 770-773.
- KANOE, M., IMAGAWA, H. & TODA, M., 1975. Distribution of Fusobacterium necrophorum in bovine alimentary tracts. Bulletin of the Faculty of Agriculture, Yamaguti University, 26, 161-172.
- KANOE, M., IMAGAWA, H., TODA, M. & SATO INOUE, M., 1976. Bacteriology of bovine hepatic abscesses. Japanese Journal of Veterinary Science, 38, 263-268
- KANOE, M., ISHII, T. & KAI, K., 1987. Effects of Fusobacterium necrophorum leukocidin on bovine ruminal cell in vitro. Microbios Letters, 35, 119-123
- KANOE, M., IZICHI, Y. & TODA, M., 1979. Isolation of Fusobacterium necrophorum from bovine ruminal lesions. Japanese Journal of Veterinary Science, 40, 275-281.
- KANOE, M. & YAMANAKA, M., 1989. Bovine platelet aggregation by Fusobacterium necrophorum. Journal of Medical Microbiology, 29, 13-17.
- KNAPPE-POINDECKER, M., GILHUUS, M., JENSEN, T. K., KLITGAARD, K., LARSSEN, R. B. & FJELDAAS, T., 2013. Interdigital dermatitis, heel ersion, and digital dermatitis in 14 Norwegian dairy herds. Journal of dairy Science, 96, 7617-7629.
- KNOTT, L., TARLTON, J. F., CRAFT, H. & WEBSTER, A. J., 2007. Effects of housing, parturition and diet change on the biochemistry and biomechanics of the support structures of the hoof of dairy heifers. Veterinary Journal, 174, 277-287.
- KOLB, V. E., 1979. Ernährungsbiochemische und pathobiochemische Aspekte der Bildung und Resorption von Endotoxinen in den Vormägen, unter besonderer Berücksichtigung der Verhältnisse bei der Parakeratose, bei der Azidose und bei der Ausbildung von Leberabszessen. Monatsschriftung für Veterinärmedicin, 34, 914-918.
- KOPP, P. A., S., D. I., J., D., M., S., B., G. & BLOBEL, H., 1996. Estreptomicina aumenta a aderencia em celulas epiteliais de Bacteroides melaninogenicus associado as lesoes peridentarias da ‘cara inchada’ dos bovinos. Pesquisa Veterinaria Brasileira, 16, 53-57.
- LAING, E. A. & EGERTON, J. R., 1978. The occurrence, prevalence and transmission of Bacteroides nodosus infection in cattle. Research in Veterinary Science, 24, 300-304.
- LANGWORTH, B. F., 1977. Fusobacterium necrophorum: Its characteristics and role as an animal pathogen. Bacteriological Reviews, 41, 373-390.
- LAVEN, R. A., VERMUNT, J. J. & MALMO, J., 2019. Lameness: causes and management. In: Parkinson TJ, Vermunt JJ, Malmo J and Laven RA (eds.), Diseases of Cattle in Australasia, 2nd edition, Auckland, New Zealand: Massey University Press.
- LECHTENBERG, K. F., NAGARAJA, T. G., LEIPOLD, H. W. & CHENGAPPA, M. M., 1988. Bacteriologic and histologic studies of hepatic abscesses in cattle. American Journal of Veterinary Research, 49, 58-62.
- LIBERG, P. & JÖNSSON, G., 1993. Ultrasonography and determination of proteins and enzymes in blood for the diagnosis of liver abscesses in intensively fed beef cattle. Acta Veterinaria Scandinavica, 34, 21-28.
- MAAS, J., DAVIS, L. E., HEMSTEAD, C., BERG, J. N. & HOFFMAN, K. A., 1984. Efficacy of ethylenediamine dihydriodide in the prevention of naturally occurring foot rot in cattle. American Journal of Veterinary Research, 45, 2347-2350.
- MACIVOR, K. M., F., D. & HORAK, I. G., 1987. Foot abscess in goats in relation to the seasonal abundance of adult Amblyomma hebraeum and adult Rhipicephalus glabroscutatum (Acari: Ixodidae). Journal of the South African Veterinary Association, 58, 113-118.
- MACKIE, R. I., GILCHRIST, F. M. C. & HEATH, S., 1984. An in vitro study of ruminal microorganisms influencing lactate turnover and its contribution to volatile fatty acid production. Journal of Agricultural Science (Cambridge), 103, 37-51.
- MADIN, S. H., 1949. A bacteriologic study of bovine liver abscesses. Veterinary Medicine, 44, 248-251.
- MADSEN, M., SORENSEN, G. H., AALBAEK, B., HANSEN, J. W. & BJORN, H., 1992. Summer mastitis in heifers: Studies on the season occurrence of Actinomyces pyogenes, Peptostreptococcus indolicus and Bacteroidaceae in clinical healthy cattle in Denmark. Veterinary Microbiology, 30, 243-255.
- MARTENS, R. G., AUER, J. A. & CARTER, K. C., 1986. Equine pediatrics: Septic arthritis and osteomyelitis. Journal of the American Veterinary Medical Association, 188, 582-585.
- MCCORMACK, J. E., 1973. Papilledema related to left cerebral hemisphere abscess in a heifer. Veterinary Medicine Small Animal Clinician, 68, 1249-1252.
- MCFADYEAN, M. J., 1891. Disseminated necrosis of the liver of the ox and sheep. Journal of Comparative Pathology and Therapeutics, 4, 346-353.
- MCLENNAN, M. W., 1988. Incidence of lameness requiring veterinary treatment in dairy cattle in Queensland. Australian Veterinary Journal, 65, 144-146.
- MGASA, M. N., 1987. Foot rot in cattle in Morogoro, Tanzania. Bulletin of Animal Health and Production in Africa, 35, 332-335.
- MILLS, K., MCCLENAUGHAN, P., MORTON, A., ALLEY, D., LIEVAART, J., WINDSOR, P. A. & EGERTON, J. R., 2012. Effect on time in quarantine of the choice of program for eradication of footrot from 196 sheep flocks in southern New South Wales. Australian Veterinary Journal, 90, 14-19 [ISSN 0005-0423].
- MORGAN, K., 1987. Foot rot. In Practice, 124-129.
- MURNANE, D., 1933. Foot rot in sheep. Journal of the Council for Scientific and Industrial Research of Australia, 6, 252-259.
- MYERS, L. L., SHOOP, D. S. & BYARS, T. D., 1987. Diarrhea associated with enterotoxic Bacteroides fragilis in foals. American Journal of Veterinary Research, 48, 1565-1567.
- NAGARAJA, T. G., BARTLEY, E. E. & FINA, L. R., 1978. Evidence of endotoxins in the rumen bacteria of cattle fed hay or grain. Journal of Animal Science, 47, 226-234.
- NAGARAJA, T. G. & LECHTENBERG, K. F., 2007. Liver abscesses in feedlot cattle. Veterinary Clinics of North America: Food Animal Practice, 23, 351-369.
- NAKAJIMA, Y., UEDA, H. & TAKEUCHI, S., 1988. Synergistic effects of Fusobacterium necrophorum lipopolusaccharide, cytoplasmic and cultural supernatant fractions on induction of acute necrosis in rabbits. American Journal of Veterinary Research, 49, 125-129.
- NAKAJIMA, Y., UEDA, H., TAKEUCHI, S. & FUJIMOTO, Y., 1987. The effects of Escherichia coli endotoxin as a trigger for hepatic infection in rabbits with Fusobacterium necrophorum. Journal of Comparative Pathology, 97, 207-215.
- NEWSOM, L. E., 1938. A bacteriologic study of liver abscesses in cattle. Journal of Infectious Diseases, 63, 232-233.
- NEWSOME, R. F., GREEN, M. J., BELL, N. J., BOLLARD, N. J., MASON, C. S., WHAY, H. R. & HUXLEY, J. N., 2017a. A prospective cohort study of digital cushion and corium thickness. Part 1: Associations with body condition, lesion incidence, and proximity to calving. Journal of Dairy Science, 100, 4745-4758.
- NEWSOME, R. F., GREEN, M. J., BELL, N. J., BOLLARD, N. J., MASON, C. S., WHAY, H. R. & HUXLEY, J. N., 2017b. A prospective cohort study of digital cushion and corium thickness. Part 2: Does thinning of the digital cushion and corium lead to lameness and claw horn disruption lesions? Journal of Dairy Science, 100, 4759-4771.
- NILSSON, S. A., 1963. Clinical, morphological and experimental studies of laminitis in cattle. Acta Veterinaria Scandinavica (Supplement), 4, 124-139.
- ORSEL, K., PLUMMER, P., SHEARER, J., DE BUCK, J., CARTER, S. D., GUATTEO, R. & BARKEMA, H. W., 2017. Missing pieces of the puzzle to effectively control digital dermatitis. Published on-line: https://doi.org?10.1111/tbed.12729.
- OSBORNE, H. G., 1950. Foot-rot in pigs. Australian Veterinary Journal, 26, 316-317.
- PARSONSON, I. M., EGERTON, J. R. & ROBERTS, D. S., 1967. Ovine interdigital dermatitis. Journal of Comparative Pathology, 77, 309-313.
- PENNY, R. H. C., CAMERON, R. D. A., JOHNSON, S., KENYON, P. J., SMITH, H. A., BELL, A. W. P., COLE, J. P. L. & TAYLOR, J., 1980. Foot rot of pigs: The influence of biotin supplementation on foot lesions in sows. Veterinary Record, 107, 350-351.
- PENNY, R. H. C., OSBORNE, A. D. & WRIGHT, A. I., 1963. The causes and incidence of lameness in store and adult pigs. Veterinary Record, 75, 1225-1240.
- PETERSEN, G. C. & NELSON, D. R., 1984. Foot diseases in cattle: Part II. Diagnosis and treatment. The Compendium of Continuing Education, 5565-5573.
- PIREZ, S., HURTADO, A., VALLE, J., MATEO, E. M., MARTIN-PALLOMINO, P. & VADILLO, S., 1996. Bacteriological study of footrot in pigs: a preliminary note. Veterinary Record, 139, 17-19.
- RÄBER, M., SCHEEDER, M. R., OSSENT, P., LISCHER, C. H. J. & GEYER, H., 2006. The content and composition of lipids in the digital cushion of the bovine claw with respect to age and location-a preliminary report. Veterinary Journal, 172, 173-177.
- RADOSTITS, O. M., GAY, C. C., BLOOD, D. C. & HINCHCLIFF, K. W., 2000. Periodontal disease. Cara inchada. In: Veterinary Medicine – A Textbook of the Diseases of Cattle, Sheep, Pigs and Horses, 9th edition, London, UK: W.B.Saunders Company Ltd.
- RAUTENBACH, G. H., 1985. The incidence of clinical cases in a peri-urban farm animal practice. Journal of the South African Veterinary Association, 56, 85-88.
- READ, D. H., WALKER, R. L., CASTRO, A. E., SUNDBURG, J. P. & THURMOND, M. C., 1992. An invasive spirochaete associated with interdigital papilomatosis of dairy cattle. Veterinary Record, 130, 59-60.
- REBHUN, W. C. & PEARSON, E. G., 1982. Clinical management of the bovine foot problems. Journal of the American Veterinary Medical Association, 181, 572–577.
- REED, G. A., 1986. The role of foot rot vaccines in Australia. In: STEWART, D. J., PETERSON, J. E., MCKERN, N. M. & EMERY, D. L., (eds.). Foot rot in Ruminants, Proceedings of a Workshop, Melbourne 1985, CSIRO Division of Animal Health, Australian Wool Corporation, Australia.
- RENDELL, D. K. & CALLINAN, A. P. L., 1997. Comparison of erythromycin and oxytetracycline for the treatment of virulent foot rot in grazing sheep. Australian Veterinary Journal, 75, 354
- ROBERTS, D. S., 1967b. The pathogenic synergy of Fusiformis necrophorus and Corynebacterium pyogenes. Part II. The response of F. necrophorus to a filterable product of C. pyogenes. British Journal of Experimental Pathology, 48, 674-679.
- ROBERTS, D. S. & EGERTON, J. R., 1969. The aetiology and pathogenesis of ovine foot rot. II. The pathogenic association of Fusiformis nodosus and F. necrophorum. Journal of Comparative Pathology, 79, 217-227.
- ROBERTS, D. S., GRAHAM, N. P. H., EGERTON, J. R. & PARSONSON, I. M., 1968. Infective bulbar necrosis (heel-abscess) of sheep, a mixed infection with Fusiformis necrophorus and Corynebacterium pyogenes. Journal of Comparative Pathology, 78, 1-8.
- ROBINSON, T. J., JASPER, D. E. & GUILBERT, H. R., 1951. The isolation of Spherophorus necrophorus from the rumen together with some feed lot data on abscess and telangiectasis. Journal of Animal Science, 10, 733-741.
- ROGERS, J. A., BRANINE, M. A., MILLER, C. R., WRAY, M. I., BARTLE, S. J., PRESTON, R. L., GILL, D. R., PRITCHARD, R. H., STILBORN, R. P. & BECHTOL, D. T., 1995. Effects of dietary virginiamycin on performance and liver abscess incidence in feedlot cattle. Journal of Animal Science, 73, 9-20.
- RUNNELS, R. A., MONLUX, W. S. & MONLUX, A. W., 1960. Principles of Veterinary Pathology. Ames, Iowa: The Iowa State University Press.
- RUSSELL, J. B. & HINO, T., 1985. Regulation of lactate production in Streptococcus bovis: A spiraling effect that contributes to rumen acidosis. Journal of Dairy Science, 68, 1712-1721.
- SCANLAN, C. M. & EDWARDS, J. F., 1990. Bacteriological and pathologic studies of hepatic lesions in sheep. American Journal of Veterinary Research, 51, 363-366.
- SCANLAN, C. M., GARRET, P. D. & CAMPBELL, E. F., 1985. Ovine contagious foot rot. The Compendium on Continuing Education, 7, S15-S18.
- SCANLAN, C. M. & HATHCOCK, T. L., 1983. Bovine rumenitis-liver abscess complex: A bacteriological review. Cornell Veterinarian, 73, 288-297.
- SCOTT, G. B., 1988. Lameness and pregnancy in Friesian dairy cows. British Veterinary Journal, 144, 273-281.
- SCOTT, P. R., PENNY, C. D. & MACRAE., 2011. Cattle medicine. London: Manson Publishing Ltd.
- SELMAN, I. E., WISEMAN, A., PETRIE, L. & PIRIE, H. M., 1974. A respiratory syndrome in cattle resulting from thrombosis of the posterior vena cava. Veterinary Record, 94, 459-466.
- SIEGMUND, O. H., 1979. The Merck Veterinary Manual. 5th edn. Rahway, New Jersey: Merck Publishing Co.
- SIMON, P. C. & STOVELL, P. L., 1969. Diseases of animals associated with Sphaerophorus necrophorus: Characteristics of the organism. Veterinary Bulletin, 39, 311-315.
- SIMON, P. C. & STOVELL, P. L., 1971. Isolation of Sphaerophorus necrophorus from bovine hepatic abscesses in British Columbia. Canadian Journal of Comparative Medicine, 35, 103-106.
- SMITH, G. R., BARTON, S. A. & WALLACE, L. M., 1987. Further observations on the enhancement of the infectivity of Fusobacterium necrophorum by other bacteria. Epidemiology and Infection, 100, 305-310.
- SMITH, G. R., TILL, D., WALLACE, L. M. & NOAKES, D. E., 1989. Enhancement of the infectivity of Fusobacterium necrophorum by other bacteria. Epidemiology and Infection, 102, 447-458.
- SMITH, G. R., WALLACE, L. M. & NOAKES, D. E., 1990. Experimental observations on the pathogenesis of necrobacillosis. Epidemiology and Infection, 104, 73-78.
- SMITH, L. D. S., 1975. The Pathogenic Anaerobic Bacteria. 2nd edn. Illinois: Charles C. Thomas.
- STEWART, D. J., 1988. Foot rot of sheep. In: EGERTON, J. R., YONG, W. K. & RIFFKIN, G. G., (eds.). Foot rot and Foot Abscess of Ruminants. Florida: CRC Press.
- STEWART, D. J., CLARK, B. L. & JARRETT, R. G., 1984. Differences between strains of Bacteroides nodosus in their effects on the severity of foot rot, bodyweight and woolgrowth in Merino sheep. Australian Veterinary Journal, 61, 348-352.
- STEWART, D. J., PETERSON, J. E., VAUGHAN, J. A., CLARK, B. L., EMERY, D. L., CALDWELL, J. B. & KORTT, A. A., 1986. Clinical and laboratory diagnosis of benign, intermediate and virulent strains of Bacteroides nodosus. In: STEWART, D. J., PETERSON, J. E., MCKERN, N. M. & EMERY, D. L., (eds.). Foot rot in Ruminants. Proceedings of a Workshop, Melbourne 1985, CSIRO Division of Animal Health, Australian Wool Corporation, Australia.
- SULLIVAN, L. E., CARTER, S. D., BLOWEY, R., DUNCAN, J. S., GROVE-WHITE, D. & EVANS, N. J., 2013. Digital dermatitis in beef cattle. Veterinary Record 173, 582.
- SWEENEY, C. R., DIVERS, T. J. & BENSON, C. E., 1985. Anaerobic bacteria in 21 horses with pleuropneumonia. Journal of the American Veterinary Medical Association, 187, 721-724.
- TAKEUCHI, S., NAKAJIMA, Y. & HASHIMOTO, K., 1983. Pathogenic synergism of Fusobacterium necrophorum and other bacteria in formation of liver abscess in BALB/c mice. Japanese Journal of Veterinary Science, 45, 775-781.
- TARLTON, J. F., HOLAH, D. E., EVANS, K. M., JONES, S., PEARSON, G. R. & WEBSTER, A. J., 2002. Biomechanical and histopathological changes in the support structures of bovine hooves around the time of first calving. Veterinary Journal, 163, 196-204.
- TAYLOR, D. J., 1989. Pig Diseases. Cambridge: The Burlington Press (Cambridge) Ltd.
- THEILER, G., 1962. The Ixodoidea parasites of vertebrates in Africa south of the Sahara (Ethiopian Region). Project S 9958. Report to the Director of Veterinary Services, Onderstepoort.
- THEILER, G. & ROBINSON, B. N., 1953. Ticks in the South African Zoological Survey Collection. Part VIII. Six lesser known African rhipicephalids. Onderstepoort Journal of Veterinary Research, 26, 93-136.
- THORLEY, C. M., CALDER, H. A. M. & HARRISON, W. J., 1977. Recognition in Great Britain of Bacteroides nodosus in foot lesions in cattle. Veterinary Record, 100, 387.
- THOROLD, P. W., 1964. Some common bacterial infections of sheep in South Africa. Journal of the South African Veterinary Medical Association, 35, 549-565.
- TODD, G. C. & KROOK, L., 1966. Nutritional hepatic necrosis in beef cattle. Sawdust liver. Pathologica Veterinaria, 3, 379-400.
- TOUSSAINT-RAVEN, E., 1973. Lameness in cattle and foot care. Netherlands Journal of Veterinary Science, 5, 2.
- TOUSSAINT-RAVEN, E. & CORNELISSE, J. L., 1971. Specific contagious inflammation of the interdigital skin in cattle. Veterinary Medical Review, 2/3, 223-247.
- TRANTER, W. P. & MORRIS, R. S., 1991. A case study of lameness in three dairy herds. New Zealand Veterinary Journal, 39, 88-96
- VAN TONDER, E. M., 1975. Notes on some disease problems in Angora goats in South Africa. Veterinary Medical Review, 109-138.
- VAN TONDER, E. M., 1983. Foot infections and other conditions of small stock. Ugqira, 16, 19.
- VAN TONDER, E. M., KELLERMAN, G. E. & BOLTON, T. F. W., 1976. An outbreak of diphtheria in boergoat kids. Journal of the South African Veterinary Association, 47, 123-124.
- VENNING, C. M., CURTIS, M. A. & EGERTON, J. R., 1990. Treatment of virulent foot rot with lincomyin and spectinomycin. Australian Veterinary Journal, 67, 258-260
- VERMUNT, J. J., 2005. Unpublished data.
- VERMUNT, J. J., HOUSE, J. H. & MALMO, J., 2019. Respiratory conditions. In: PARKINSON, T. J., VERMUNT, J. J., MALMO, J. & LAVEN, R. A., (eds.). Diseases of Cattle in Australasia, 2nd edition, Auckland, New Zealand: Massey University Press.
- VERMUNT, J. J. & MALMO, J., 2019. Diseases of the hepatobiliary system. In: PARKINSON, T. J., VERMUNT, J. J., MALMO, J. & LAVEN, R. A., (eds.). Diseases of Cattle in Australasia, 2nd edition, Auckland, New Zealand: Massey University Press.
- WAGENAAR, G., 1963. Trombose van de vena cava posterior bij het rund. Tijdschrift voor Diergeneeskunde, 88, 30-33.
- WALKER, J. B., 1990. Two new species of ticks from southern Africa whose adults parasitize the feet of ungulates: Rhipicephalus lounsburyi n. sp. and Rhipicephalus neumanni n. sp. (Ixodoidea, Ixodidae). Onderstepoort Journal of Veterinary Research, 57, 57-75.
- WALKER, R., 1990. Foot rot Technical Information Manual. 2nd edn. New South Wales Department of Agriculture and Fisheries, Australia.
- WEAVER, A. D., 1974. Lameness in cattle: The interdigital space. Veterinary Record, 95, 115-120.
- WEAVER, A. D., 1988. Cattle foot problems. Part 1. Introduction and interdigital skin disease. Agri-Practice, 9, 34-38.
- WEAVER, A. D., 1988. Cattle foot problems. Part 2: Diseases of the horn and corium. Agri-Practice, 9, 35-40.
- WEAVER, A. D., ANDERSON, L., DE LAISTRE BANTING, L., DEMERZIS, P. N., KNEZEVIC, P. F., PETERSE, D. J. & SANKOVIC, F., 1981. Review of disorders of the ruminant digit with proposals for anatomical and pathological terminology and recording. Veterinary Record, 108, 117-120.
- WEBB WARE, J. K., SCRIVENER, C. J. & VIZARD, A. L., 1994. Efficacy of erythromycin compared with penicillin/streptomycin for the treatment of virulent foot rot in sheep. Australian Veterinary Journal, 71, 88-89.
- WEST, D. M., 1981. A study of foot abscess in sheep. PhD thesis, Massey University, New Zealand
- WEST, D. M., 1983. Observations on an outbreak of foot abscess in sheep. New Zealand Veterinary Journal, 31, 71-74.
- WEST, D. M., 1989. Foot abscess in sheep. In: EGERTON, J. R., YONG, W. K. & RIFFKIN, G. G., (eds.). Foot rot and Foot Abscess of Ruminants. CRC Press.
- WEST, D. M., 1990. Foot abscess and other lameness problems of sheep. In: Sheep Medicine. Proceedings of the Sandy and Georgina Reid Memorial Refresher Course for Veterinarians, 16-20 July 1990, University of Sydney, Australia.
- WESTRA, R., 1981. Hoof problems in cattle. Is there a relationship with trace mineral levels? The Second Western Nutrition Conference, Edmonton, Alberta, Canada, 114–132.
- WHITTINGTON, R. J., 1996. Further observations on the primary and anamnestic humoral responses to Dichelobacter nodosus in sheep in relation to the diagnosis of foot rot. Research in Veterinary Science, 60, 126-133.
- WHITTINGTON, R. J. & EGERTON, J. R., 1994. Application of ELISA to the serological diagnosis of virulent ovine foot rot. Veterinary Microbiology, 41, 147-161.
- WRIGHT, A. I., OSBORNE, A. D., PENNY, R. H. C. & GRAY, E., 1972. Foot-rot in pigs: Experimental production of the disease. Veterinary Record, 90, 93-99.
- ZIENAB, E.-S., M., EL-SEEDY, F. R., EL-BARDISY, M. M. & KAMEL, M., 1991. A bacteriological study of sheep liver abscesses. Veterinary Medical Journal, Giza, 39, 91-103.




