- Infectious Diseases of Livestock
- Part 3
- Porcine pleuropneumonia
- GENERAL INTRODUCTION: SPIROCHAETES
- Swine dysentery
- Borrelia theileri infection
- Borrelia suilla infection
- Lyme disease in livestock
- Leptospirosis
- GENERAL INTRODUCTION: AEROBIC ⁄ MICRO-AEROPHILIC, MOTILE, HELICAL ⁄ VIBROID GRAM-NEGATIVE BACTERIA
- Genital campylobacteriosis in cattle
- Proliferative enteropathies of pigs
- Campylobacter jejuni infection
- GENERAL INTRODUCTION: GRAM-NEGATIVE AEROBIC OR CAPNOPHILIC RODS AND COCCI
- Moraxella spp. infections
- Bordetella bronchiseptica infections
- Pseudomonas spp. infections
- Glanders
- Melioidosis
- Brucella spp. infections
- Bovine brucellosis
- Brucella ovis infection
- Brucella melitensis infection
- Brucella suis infection
- Brucella infections in terrestrial wildlife
- GENERAL INTRODUCTION: FACULTATIVELY ANAEROBIC GRAM NEGATIVE RODS
- Klebsiella spp. infections
- Escherichia coli infections
- Salmonella spp. infections
- Bovine salmonellosis
- Ovine and caprine salmonellosis
- Porcine salmonellosis
- Equine salmonellosis
- Yersinia spp. infections
- Haemophilus and Histophilus spp. infections
- Haemophilus parasuis infection
- Histophilus somni disease complex in cattle
- Actinobacillus spp. infections
- Actinobacillus equuli infections
- Gram-negative pleomorphic infections: Actinobacillus seminis, Histophilus ovis and Histophilus somni
- Porcine pleuropneumonia
- Actinobacillus suis infections
- Pasteurella and Mannheimia spp. infections
- Pneumonic mannheimiosis and pasteurellosis of cattle
- Haemorrhagic septicaemia
- Pasteurellosis in sheep and goats
- Porcine pasteurellosis
- Progressive atrophic rhinitis
- GENERAL INTRODUCTION: ANAEROBIC GRAM-NEGATIVE, IRREGULAR RODS
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: GRAM-POSITIVE COCCI
- Staphylococcus spp. infections
- Staphylococcus aureus infections
- Exudative epidermitis
- Other Staphylococcus spp. infections
- Streptococcus spp. infections
- Strangles
- Streptococcus suis infections
- Streptococcus porcinus infections
- Other Streptococcus spp. infections
- GENERAL INTRODUCTION: ENDOSPORE-FORMING GRAM-POSITIVE RODS AND COCCI
- Anthrax
- Clostridium perfringens group infections
- Clostridium perfringens type A infections
- Clostridium perfringens type B infections
- Clostridium perfringens type C infections
- Clostridium perfringens type D infections
- Malignant oedema⁄gas gangrene group of Clostridium spp.
- Clostridium chauvoei infections
- Clostridium novyi infections
- Clostridium septicum infections
- Other clostridial infections
- Tetanus
- Botulism
- GENERAL INTRODUCTION: REGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Listeriosis
- Erysipelothrix rhusiopathiae infections
- GENERAL INTRODUCTION: IRREGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Corynebacterium pseudotuberculosis infections
- Corynebacterium renale group infections
- Bolo disease
- Actinomyces bovis infections
- Trueperella pyogenes infections
- Actinobaculum suis infections
- Actinomyces hyovaginalis infections
- GENERAL INTRODUCTION: MYCOBACTERIA
- Tuberculosis
- Paratuberculosis
- GENERAL INTRODUCTION: ACTINOMYCETES
- Nocardiosis
- Rhodococcus equi infections
- Dermatophilosis
- GENERAL INTRODUCTION: MOLLICUTES
- Contagious bovine pleuropneumonia
- Contagious caprine pleuropneumonia
- Mycoplasmal pneumonia of pigs
- Mycoplasmal polyserositis and arthritis of pigs
- Mycoplasmal arthritis of pigs
- Bovine genital mycoplasmosis
- Neurotoxin-producing group of Clostridium spp.
- Contagious equine metritis
- Tyzzer's disease
- MYCOTIC AND ALGAL DISEASES: Mycoses
- MYCOTIC AND ALGAL DISEASES: Pneumocystosis
- MYCOTIC AND ALGAL DISEASES: Protothecosis and other algal diseases
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Epivag
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ulcerative balanoposthitis and vulvovaginitis of sheep
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ill thrift
- Eperythrozoonosis
- Bovine haemobartonellosis
Porcine pleuropneumonia
This content is distributed under the following licence: Attribution-NonCommercial CC BY-NC  View Creative Commons Licence details here
View Creative Commons Licence details here
Porcine pleuropneumonia
M-L PENRITH AND M M HENTON
Introduction
Porcine pleuropneumonia, caused by Actinobacillus pleuropneumoniae, is a highly contagious and often fatal disease that most often affects pigs aged between 12 and 15 weeks, although animals of all ages are susceptible.27, 55, 69, 81, 82 It may manifest clinically as a peracute, acute, subacute or chronic disease, the more acute forms being characterized by the presence of a fibrinous to fibrinonecrotic bronchopneumonia, and the chronic by the development of pulmonary sequestra and reduced weight gain. Pigs that survive acute disease, as well as healthy animals that have never developed clinical signs of the disease, may be carriers of the infection.17, 55
A Haemophilus-like organism was first described from cases of porcine pleuropneumonia in England in 1957.61 Since the late 1960s, porcine pleuropneumonia has been of major economic importance in European countries, particularly Scandinavia,69 and has also become increasingly important to the pig industry in many countries throughout the world. In South Africa the organism was isolated for the first time in 1985. In contrast to most countries where it initially caused explosive outbreaks of disease with high mortality, the first cases diagnosed in South Africa were characterized by the development of an insidious form of chronic pneumonia complicated by simultaneous infections with Pasteurella multocida, Streptococcus dysgalactiae var. dysgalactiae, Streptococcus suis or Trueperella pyogenes. Subsequently, the more typical peracute, acute, subacute and chronic forms of the disease have occurred in South Africa. Most outbreaks have almost exclusively involved pigs aged between two and six months.
Outbreaks of porcine pleuropneumonia are the cause of severe economic losses as a result of the high mortality rateand high cost of chemotherapy. The subclinical and chronic forms of the disease may result in reduced herd performance.55, 66, 82
Aetiology
The genus Actinobacillus belongs to the family Pasteurellaceae, which comprises short, Gram-negative, non-motile,non-spore-forming, pleomorphic rods, with a tendency to occur mainly in coccobacillary forms. The other two members of the family are Haemophilus and Pasteurella.
The genus Haemophilus is defined by growth factor requirements, which have also been used as a criterion for speciation within the genus.40 These, possibly plasmid-controlled, factors21 are Factor X (protoporphyrin IX or protoheme) and Factor V (nicotinamide adenine dinucleotide or NAD).
As most strains of A. pleuropneumoniae require Factor V, or Factor V-related compounds, the species was initially placed in the genus Haemophilus. However, on the basis of DNA:DNA hybridization data, it is now classified as an Actinobacillus62 and is divided into two biotypes. Biotype 1 requires Factor V and occurs worldwide. Biotype 2 is Factor V-independent (although it still appears to require Factor Vrelated compounds) and has been isolated in Switzerland, the USA, and Canada.17, 38, 50
Actinobacillus pleuropneumoniae is furthermore Factor X-independent and CAMP-positive, ferments mannitol and is β-haemolytic on 5 per cent calf- or sheep-blood agar (Table 161.1).40 It is urease-positive, but a urease-negative variant of A. pleuropneumoniae has been described.8 Actinobacillus pleuropneumoniae forms small, whitish, opaque colonies (1 to 2mm in diameter) within 48 hours of incubation on chocolate blood agar. Two types of colonies have been described: a rough, round, hard, waxy type that adheres to wire inoculating loops, and a flatter, soft and more readily serotypable, glistening colony.40 Most virulent strains are heavily capsulated and produce iridescent colonies on Levinthal agar.39
The antigenic properties of A. pleuropneumoniae have been extensively researched.12, 19, 49, 54, 58 There are antigenic, serotype-specific, membrane lipopolysaccharides and capsular polysaccharides.41 Resistance to complement-mediated host defences is due to the capsule,17 and nonencapsulated mutants are generally avirulent and rapidly cleared.32 Based on differences in the capsular polysaccharides, A. pleuropneumoniae biotype 1 is divided into 12 serotypes. 55 Common antigens (lipopolysaccharide and outer membrane proteins)32, 46, 56 exist that complicate diagnostic and epidemiological studies based on serology.59 Cross– reactions are common between serotypes 1, 9 and 11, between 4 and 7, and between 3, 6 and 8,41, 46, 56 but cross-reactivity between virtually all serotypes can occur, depending on the antigen and test method used.24 The use of monoclonal antibodies yields more specific results.48 Isolates that cannot be typed have been reported.7, 17
Table 161.1 Simplified bacteriological differentiation criteria of Actinobacillus spp. that may be isolated from pigs31
| CHARACTERISTIC | A. PLEUROPNEUMONIAE | A. SUIS | A. EQUULI | A. LIGNIERESII | |
|---|---|---|---|---|---|
| BIOVAR 1 | BIOVAR 2 | ||||
| NAD-requirement Haemolysis Urease Aesculin CAMP Trehalose Mannitol Raffinose | + + + - + - + v | – + + - + - + v | – + + + + + - - | – v + - - + + + | – - + - - - + + |
v = variable
Epidemiology
Actinobacillus pleuropneumoniae is a primary pathogen of the respiratory tract of pigs. It rarely affects other animals. The only reports of isolation from lesions in other species are a case of arthritis in a lamb and a brain abscess in a steer.36 Intensification of pig production is an important factor in the epidemiology of the disease.55
When the infection is first introduced into a herd, all age groups may be affected. With the disappearance of colostral immunity at six weeks, pigs become susceptible to the disease. 57 However, in infected herds, piglets are usually protected by colostral antibodies for one or two months, during which time they are likely to be exposed to infection, usually before 21 days of age. Clinical disease does not occur, and these piglets apparently develop lifelong immunity.17 Some may, however, become carriers due to subclinical, chronic infection. When an outbreak occurs, for example owing to the introduction of uninfected pigs into an infected herd, heavy environmental contamination may result in a sufficient number of organisms to overcome immunity and produce clinical disease.17 The apparent predilection for growing pigs of three months and older may be due to the conditions under which pigs of this age are kept, when overcrowding, poor ventilation and extremes of temperature may become important factors.55
Disease caused by A. pleuropneumoniae has been described from most countries with developed pig industries: most European countries, North and South America, Asia, Australia55 and South Africa. Although A. pleuropneumoniae occurs throughout South Africa, most cases have been reported from the high-lying inland regions of Gauteng and North-West provinces, where most of the commercial pig production occurs. Actinobacillus pleuropneumoniae has not been reported from any other African country.
The occurrence of different serotypes may be restricted to certain regions or countries. For example, serotypes 4, 9 and 11 have not been recorded in North America,38and a study in the British Isles revealed that serotype 6, common in Great Britain, was apparently absent in Ireland.44 In South Africa, serotypes 7, 8 and 3 are the most common, but serotypes 1, 2, 5, 6, 9, 10 and 12 have also been found.28
Epidemiological patterns are partly determined by the serotypes present in an area, and the introduction of new, virulent serotypes may alter that pattern from an endemic situation, with mild disease, to an epidemic situation.25 Some serotypes are more virulent than others,7, 17, 22, 34 and virulence of a particular serotype can differ between different countries.10, 14
Pigs suffering from the acute disease shed large numbers of organisms in nasal discharges and in aerosols.68 Transmission occurs mainly through the respiratory route by the inhalation of infected material and aerosols by pigs that are maintained in close contact with each other.40 All the pigs in a pen are usually affected.17 Environmental and managemental factors often contribute to the development of the disease.72, 76 Conditions conducive to aerosol formation, changes in humidity, close confinement and overcrowding —including the crowding that often occurs in cold weather — facilitate the spread of the disease among pigs. Aerosols containing small droplets are formed under conditions of low temperatures and low to medium humidity levels, and these may penetrate into the respiratory system as far as the alveoli.68, 78 Aerosol transmission can occur over distances of at least 1m.77
Pigs that have recovered from clinical disease may serve as inapparent carriers for many months or even years. In these animals, the organisms are located mainly in the tonsillar crypts and/or sequestra in the lungs, and infrequently in the nasal cavity.40, 82 In addition, in infected herds a variable number of apparently healthy pigs that have never manifested clinical signs may carry the bacterium in their tonsillar crypts and nasal cavities; in one herd as many as 53 per cent of the animals were recorded as being healthy carriers. 37 Such animals are important reservoirs of the bacterium and their introduction into susceptible herds may result in the spread of the infection,40 the appearance of overt disease usually but not always being triggered by environmentally or managementally induced stress, e.g. transportation. On account of the potentially short incubation period, susceptible animals in contact with carriers during transportation to abattoirs can develop acute pleuropneumonia and die before slaughter. An abrupt change of climate, such as a sudden increase or decrease in the prevailing environmental temperature, can also precipitate clinical disease. The prevalence of the disease in infected herds may gradually increase from a low rate in summer to a peak in winter or spring.40 In South Africa, the number of cases of pleuropneumonia peaks in the early summer.28 Prior or concurrent infection with organisms such as mycoplasmas, salmonellas, toxigenic P. multocida, porcine reproductive and respiratory syndrome (PRRS) virus and Aujeszky’s disease virus that reduce the respiratory defences tends to increase the severity of A. pleuropneumoniae infection,17, 67 although the effect of PRRS virus has been disputed.63
The organism is susceptible to common disinfectants such as 2 per cent chlorine dioxide fogging, desiccation and sunlight.68 It is unlikely to survive for longer than a day in the environment,51 and it is therefore probably not disseminated mechanically by vectors. It can, however, survive for a few days in organic matter, such as nasal discharges and mucus,55 and, because of the massive nasal excretion of exudate during the acute phase of the disease, indirect transmission by fomites and farm personnel cannot be excluded.55
Pathogenesis
The pathogenesis of A. pleuropneumoniae has not been fully elucidated, but various studies have demonstrated how damage to lung tissue occurs. The upper respiratory tract and tonsillar crypts are primary sites of infection. The immune status of the pig determines the number of organisms required to cause clinical disease.17 Several factors that permit the bacteria to gain access to the lungs and cause clinical disease have been identified.
Suppression of the mucociliary escalator appears to favour infection of the lungs, presumably by permitting more organisms to reach them.53 Bacteria reach the lungs from primary sites of infection or directly through deep inhalation of infected aerosols. Dissemination of the bacteria is via lymphatics53 and possibly oedema fluid as well.2 Lesions develop as a result of the direct effects of the bacteria on host cells as well as the host’s inflammatory response. Direct damage will be limited by the host’s ability to phagocytose and kill bacteria and to neutralize secreted toxins. An excessive host response may, however, lead to severe lesions. If large numbers of bacteria are killed, endotoxic shock may occur.
It has been shown that lipopolysaccharide is chiefly responsible for adhesion of A. pleuropneumoniae to porcine respiratory tract cells and mucus.65 Fimbriae have been demonstrated but their role in adhesion is unknown.11, 26 Adhesion is considered to be an important initial step in the pathogenesis as it permits high local concentration of toxins.26
In situ hybridization has demonstrated that A. pleuropneumoniae primarily infects neutrophils and macrophages.45 Secreted protein toxins named Apx I, II and III have been proven to be very important in causing the observed effects of A. pleuropneumoniae on lung tissue. They cause haemolysis and kill alveolar macrophages; I and II are both haemolytic and cytotoxic, while III is only cytotoxic.12
Toxin production varies between serotypes, which may produce one or two of the three proteins. In an experimental study, low concentrations of haemolytic and cytotoxic Apx caused severe irreversible swelling of alveolar macrophages, resulting in impaired chemotaxis, attachment and phagocytosis. 74 Much higher doses were needed for cytolysis. Another study demonstrated that haemolysin produced by A. pleuropneumoniae inhibited phagocytosis of the bacteria by neutrophils via its cytotoxic effect.80 Bacterial surface components, including lipopolysaccharide and outer membrane proteins, have been demonstrated to be cytotoxic in vitro30 and are believed to act synergistically with secreted protein toxins to cause lung lesions.
Other contributors to lesion development in porcine pleuropneumonia are inflammatory cytokines, particularly IL-1 and IL-8, which may be released in large quantities as a result of excessive host response,4 and endotoxin,17 which may explain the vascular effects, such as intravascular coagulation.
The pathogenic process is modified by the presence of antibodies, so that disease may be mild or inapparent. Pigs that have been exposed to natural infection develop circulating antibodies within 10 to 14 days, which appear to protect against all serotypes, probably because they are produced in response to the entire spectrum of immunogenic factors. Antibodies against specific antigens, such as lipopolysaccharide and Apx, offer only partial, and often serotype- specific, immunity.
Clinical signs
The incubation period may vary from a few hours to a few days,55 depending on the size of the infective dose and the susceptibility of the host.
In susceptible herds with no natural immunity, and especially if predisposing factors are present, the peracute and acute forms usually occur. Spread is rapid, with fatalities occurring in all age groups. Morbidity of more than 50 per cent, with 1 to 10 per cent mortality is usual,17 but mortality rates of 20 to 80 per cent are possible.16
The first signs in peracutely affected pigs are usually a sudden loss of appetite and a high rectal temperature (up to 41,5 °C).55 Some individuals die within four hours of infetion, without clinical signs having been observed. Other signs in the peracute disease include cyanosis of the skin and mucous membranes, dyspnoea, respiratory distress, a moist suppressed cough, vomition, slight diarrhoea, epistaxis and, terminally, a copious, foamy, blood-tinged discharge from the mouth and nostrils.55, 58 Death usually occurs within 24 to 36 hours of the onset of the disease. Neonatal piglets usually develop fatal septicaemia.55
Acute cases begin with high fever (40,5 to 41 °C), and lethargy, stiffness, lameness and anorexia may be observed. 17, 55 As the disease progresses, pigs show signs of respiratory distress and dyspnoea when forced to move. A short, suppressed cough may be heard. The disease may lead to death in one or two days, or may proceed to the subacute and chronic stage.55, 73 Pregnant sows may abort as a sequel to the acute disease.55
Pigs with subclinical and chronic infection may show no characteristic clinical signs. Loss of appetite may result in reduced food intake and retarded growth rate.66 They may suffer from a chronic cough and sometimes an elevated body temperature. The presence of the lung lesions may exacerbate the clinical signs caused by other concurrent respiratory infections.55
Sequelae after septicaemic spread of the organism include arthritis, endocarditis, and abscess formation in the lungs, which occur more commonly after infection with serotype 3 than with the other serotypes.55 Fibrinopurulent arthritis and osteomyelitis have been described in fattening pigs after infection with serotype 2. 75 Otitis media in a weaned pig that exhibited characteristic vestibular signs has also been ascribed to infection with A. pleuropneumoniae. 15
Pathology
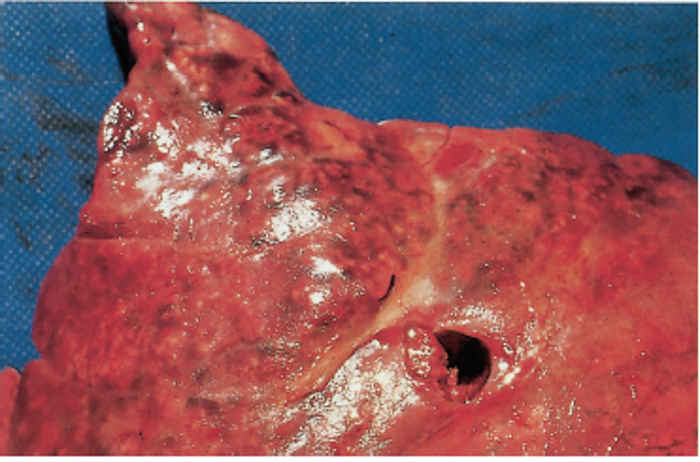
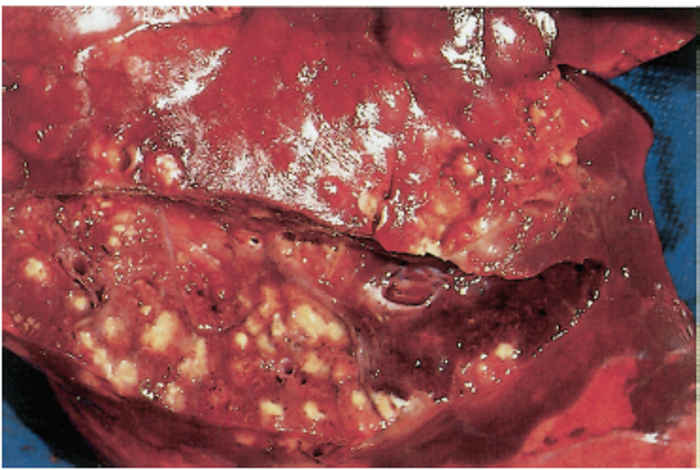
Gross and microscopic pathology vary according to the nature and course of the disease, but the most prominent lesions are usually found in the upper respiratory tract and thoracic cavity.16, 52, 60 In the peracute and acute forms, blood-tinged, frothy exudate may ooze from the nares and fill the upper respiratory passages. The mucosa of the nasal cavity, trachea and bronchi is congested, and may contain haemorrhages. The development of lung lesions depends on the duration of the disease, but the lesions are usually characterized by oedema and extensive areas of haemorrhagic to fibrinonecrotic pneumonia (Figure 161.1 and Figure 161.2), accompanied by fibrinous pleuritis. Pneumonic foci are not restricted to the cranioventral parts of the lung, and commonly occur in the dorsocaudal and hilar regions, probably owing to the virulence of the organism and the effects of vasculitis.16 Serosanguineous hydrothorax and hydropericardium, and fibrinous pericarditis are frequently present. The intrathoracic lymph nodes are enlarged but not haemorrhagic. 5, 52, 60
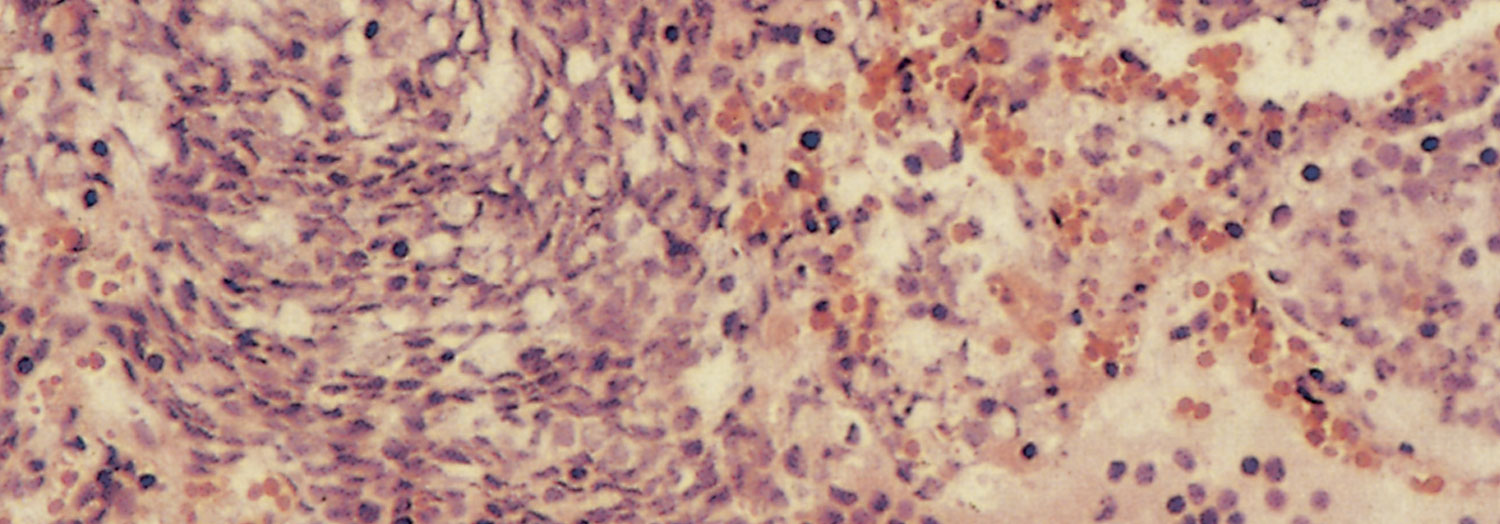
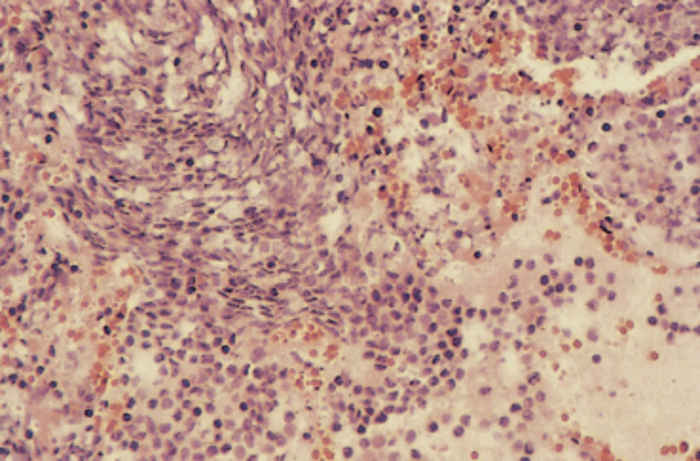
Microscopically in peracutely affected animals there is congestion, haemorrhage, oedema and serofibrinous exudate in the alveoli and interstitial tissues of the lungs (Figure 161.3). Cell infiltrates consist of mononuclear cells and neutrophils. 2
In pigs that survive longer, irregular areas of haemorrhage with necrosis and loss of architecture may be observed, with oedema and fibrin exudation into alveoli and septa.2 Round and fusiform cells believed to originate from neutrophils,2sometimes arranged in a swirling pattern, surround blood and lymph vessels, bronchioles and necrotic lesions. Alveoli may contain neutrophils and macrophages. The pleura and septa are thickened as a result of oedema and fibrin accumulation containing a mixed infiltrate of neutrophils and macrophages. Vascular lesions, including fibrinoid necrosis and intravascular fibrin are usually present and may occur in other organs, particularly the kidneys.16
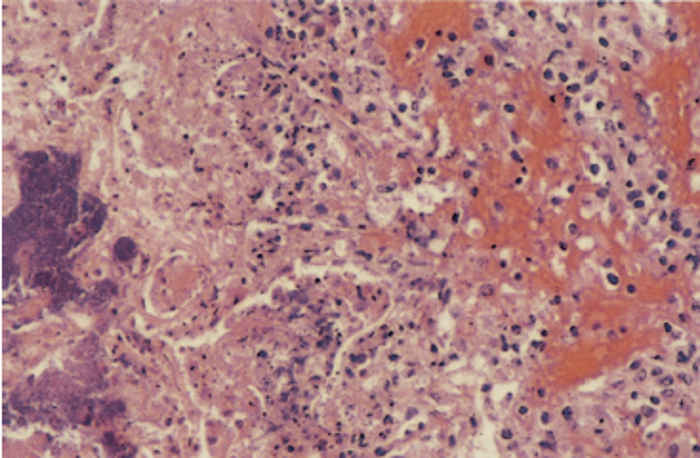
Subacute cases are characterized by areas of coagulative to lytic necrosis encapsulated by fibrosis. Swirling patterns of cells surrounding necrotic zones are more prominent (Figure 161.4).2
Other microscopic lesions that have been described include marked epithelial desquamation with subepithelial infiltration of neutrophils and mononuclear cells in the trachea and bronchi, and changes in regional lymphoid tissue that vary from depletion in peracute and acute cases to follicular hyperplasia with perifollicular infiltration of neutrophils in cases that survive infection and develop subacute lesions.2 Fibrinopurulent to fibrinonecrotic lesions have been described in cases of arthritis, osteomyelitis and otitis media.15, 35
Lesions in the lungs may resolve completely in pigs that recover from the disease, but often small, encapsulated pulmonary sequestra remain in which the causative organisms persist, accounting largely for the carrier state of the disease. 2 If the sequestra become secondarily invaded, for example by T. pyogenes, P. multocida or streptococci, they may be transformed into abscesses. Chronic lung lesions and fibrous pleuritis may be found at slaughter in apparently healthy pigs. Unless A. pleuropneumoniae can be detected, these lesions cannot be distinguished from those caused by many other pulmonary pathogens of swine.17, 79
Diagnosis
A presumptive diagnosis of porcine pleuropneumonia can be made on the clinical signs, necropsy and histopathological findings, but isolation of A. pleuropneumoniae is necessary to confirm it.
Specimens for bacteriological examination from fatal cases of the more acute disease should comprise tissue samples of lung lesions and bronchial and mediastinal lymph nodes. Specimens from the lungs should preferably be taken from lesions in the caudal lobes, as they tend to contain fewer contaminants than those in the cranial lobes. Recovery of the organism from other tissues and organs, even when the disease is septicaemic, tends to be erratic.
It is generally easier to recover A. pleuropneumoniae from the affected tissues of more acute cases, because in subacute and chronic lesions it may have been overgrown or even killed by other species of bacteria, such as P. multocida, alpha and beta haemolytic streptococci, and T. pyogenes, 29, 82 and a definitive diagnosis is not always possible.
The organism may also be isolated from swabs of nasal discharges in live animals, from the joint fluid of joints affected by arthritis,29, 75 and from the tonsillar crypts. In the latter case, the material for bacteriological culture should preferably originate from the tissue side rather than from the pharyngeal side in order to minimize contamination.
Actinobacillus pleuropneumoniae usually survives in swabs and sampled tissue or exudate for at least four days under various storage conditions at temperatures lower than 20 °C. Apart from possible co-infection of the lesions with other species of bacteria, its isolation may be hampered by post-mortem decomposition of affected tissues, or if the animal has been treated with an antibiotic before collection of the specimens.29 In order to overcome some of these problems, selective media37, 78 and dilution techniques have been used. Rapid detection methods, such as coagglutination, fluorescent antibody techniques48 and latex agglutination,33 have proved useful. The polymerase chain reaction (PCR) is highly sensitive and specific.17, 20, 42
Immunoperoxidase techniques2, 23, 31 are particularly useful if tissue has been fixed in formalin, and to observe the distribution of antigen.
Once isolated, the strain may be serotyped. Several colonies should be chosen, as more than one strain may be present. A number of techniques for serotyping have been described, including tube and slide agglutination, ring and slide precipitation, counterimmunoelectrophoresis, indirect haemagglutination, coagglutination, immunodiffusion, and immunofluorescence.38 Whilst coagglutination and slide agglutination are the tests usually used for routine typing, immunodiffusion and indirect haemagglutination tests give more conclusive results.56 The use of a panel of monoclonal antibodies and the dot ELISA have proved rapid and accurate.38 The coagglutination test has the advantage that antigen can be detected directly from lung samples of pigs with acute or chronic respiratory problems, and from those of apparently healthy carriers.48 Type-specific and multiplex PCR tests are likely to become the tests of choice in the future, as they can be performed on isolates or tissue samples.42
To determine whether a herd is infected, serological and bacteriological screening may be carried out on a number of slaughtered pigs. Examination of the lungs for lesions of chronic pneumonia rarely results in a definitive diagnosis of pleuropneumonia caused by A. pleuropneumoniae, since the lesions are difficult to distinguish from those caused by other organisms, such as P. multocida.17, 79 The success of isolation of from such lesions, even when experimentally induced, is also variable.11 Furthermore, the lesions caused by A. pleuropneumoniae frequently resolve in a few weeks, and are no longer detectable at slaughter.17
Serological screening to determine antibody levels can conveniently be done using blood obtained at slaughter. The complement fixation test, which detects antibodies to surface, in particular capsular, antigens, has for a long time been the standard test.17 Its disadvantages are that it detects mainly IgM antibodies, which decrease progressively after infection, and that it does not detect non-encapsulated (untypable) strains.17 It is reasonably serotype-specific. The ELISA is more sensitive,17, 83 but the reliability of different ELISAs is variable, and the tests are generally type- or group-specific so that several may need to be performed. False positive results lead to overdiagnosis of the disease.17, 47
Detection of A. pleuropneumoniae in tonsillar tissue offers an alternative method of herd screening, and can be used in combination with serology.70 The rate of success of isolation of A. pleuropneumoniae is considerably higher in tonsillar tissue than in nasal mucosa or lung tissue.11 Sensitivity is greatly improved by the use of a PCR test, for which the bacteria need not be viable. Detection of individual carrier animals has proved difficult because serological antibodies may not be detected and isolation may fail.11, 70 Testing by PCR for bacterial antigen may be the best method to detect carriers.42
Differential diagnosis
Porcine pleuropneumonia should be differentiated from pneumonia caused by a variety of micro-organisms. Pasteurella multocida infection is probably the most important differential diagnosis, but other organisms, such as Haemophilus parasuis, Salmonella Choleraesuis, S. Typhisuis, T. pyogenes and Mycoplasma hyopneumoniae, may cause at least macroscopically and sometimes microscopically similar lesions of chronic pneumonia. Mycoplasma hyopneumoniae lesions can generally be distinguished histopathologically by lymphofollicular proliferation around bronchioles and blood vessels and in septa,18 and are often combined with lesions caused by A. pleuropneumoniae. Infections caused by S. Choleraesuis may be accompanied by multifocal, randomly disseminated foci of necrosis in the liver.79 In A. pleuropneumoniae infections, lung lesions are often prominent in the caudal as well as the cranial lobes, in contrast to most bronchopneumonias, in which lesions are usually restricted to, or at least predominant in the cranial lobes. The peracute form of A. pleuropneumoniae infection may be difficult to distinguish from other bacterial septicaemias and indeed other causes of sudden death.
Control
During an outbreak, suitable antimicrobial treatment can reduce mortality and the severity of clinical disease.17 Actinobacillus pleuropneumoniae is generally susceptible to a wide variety of antimicrobials, but resistance to various substances has been reported,3, 23, 64 and an antibiogram is recommended before treatment is initiated. However, good in vitro sensitivity may not reflect the ability of the antimicrobial to cure pleuropneumonia in vivo, since it has been suggested that the effectiveness of the treatment will depend upon the ability of the antimicrobial to penetrate alveolar macrophages.1 In South Africa, the organism is generally susceptible to ampicillin, cephalosporins and quinolones.28 Treatment of large numbers of sick pigs may prove difficult and expensive, particularly as parenteral treatment is most likely to be effective.17 Animals suffering from the chronic disease do not generally respond well to antimicrobial therapy. Treated animals may continue to harbour the organisms in pulmonary sequestra, which are usually not eliminated even by prolonged treatment with high levels of antimicrobials.40
Prophylactic measures include medication, vaccination and other management strategies. As a prophylactic measure, in-feed medication has been demonstrated to reduce the severity of clinical disease but not to prevent infection.17 Products containing the active ingredients tylosin and tilmicosin may be most effective, administered at the dosage levels recommended by the manufacturers.
Vaccination has to date yielded variable results, and vaccines that perform well under experimental conditions may not achieve similar results under natural conditions.55 Most commercial vaccines are serotype-specific71 and offer inconsistent protection. Reduction of mortality and clinical disease may be achieved but not prevention of infection.17 Vaccines that contain bacterial whole cell antigens as well as secreted toxins, are most likely to be successful,71 as they most closely mimic natural infection. The route used for vaccination may be important, and the instructions of the manufacturer should be followed.43 A vaccine against A. pleuropneumoniae has recently become available in South Africa. To date, the results appear to be as variable as observed elsewhere.
Management is the most important factor in prevention of losses due to A. pleuropneumoniae. Effective environmental control measures include good ventilation, minimizing temperature and humidity fluctuation, and an all-in, all-out system. Overcrowding and mixing of age groups appear to be very important factors that predispose to disease. Maintaining a closed herd as far as possible, with quarantine and treatment of new breeding stock, may be helpful. Knowing the status of the herd with respect to A. pleuropneumoniae infection is useful in formulating policy for introducing new stock. While it is obviously advisable to ensure that pigs introduced into uninfected herds are also free of infection, introducing fully susceptible pigs into subclinically infected herds might provoke an outbreak that will result in sufficient build-up of organisms to cause clinical disease throughout the herd. Prevention of enzootic pneumonia may be important in the prevention of porcine pleuropneumonia.84
Early weaning systems (piglets weaned before 12 days of age) have proven successful in preventing the disease.13 It has been suggested that the introduction of Hampshire breed pigs into breeding systems can reduce the incidence of respiratory tract infections.6
References
- AGERSO, H., FRIIS, C. & NIELSEN, P., 1998. Penetration of amoxycillin to the respiratory tract tissues and secretions in Actinobacillus pleuropneumoniae infected pigs. Research in Veterinary Science, 64, 251–257.
- AJITO, T., HAGA, Y., HOMMA, S., GORYO, M. & OKADA, K., 1996. Immunohistological evaluation on respiratory tract lesions of pigs intranasally inoculated with Actinobacillus pleuropneumoniae serotype 1. Journal of Veterinary Medical Science, 58, 297–303.
- ASAWA, T., KOBAYASHI, H., MITANI, K., ITO, N., MOROZUMI, T., 1995. Serotypes and antimicrobial susceptibility of Actinobacillus pleuropneumoniae isolated from piglets with pleuropneumonia. Journal of Veterinary Medical Science, 57, 757–759.
- baarsch, m.j., scamurra, r.w., burger, k., foss,d.l., maheswaran, s.k. & murtaugh, m.p., 1995. Inflammatory cytokine expression in swine experimentally infected with Actinobacillus pleuropneumoniae. Infection and Immunity, 63, 3587–3594.
- BERTRAM, T.A., 1990. Actinobacillus pleuropneumoniae: Molecular aspects of virulence and pulmonary injury. Canadian Journal of Veterinary Research, 54, S53–56.
- BESKOW, P., ROBERTSSON, J.A. & SÖMDERLIND, O., 1993. Testing of remedial measures in fattening pig herds affected with subclinical infections. Journal of Veterinary Medicine (B), 40, 549–558.
- BLACKALL, P.J. & PAHOFF, J.L., 1995. Characterisation of porcine haemophili isolated from Australian pigs between 1988 and 1992. Australian Veterinary Journal, 72, 18–21.
- BLANCHARD, P.C., WALKER, R.L. & GARDNER, I., 1993. Pleuropneumonia in swine associated with a urease-negative variant of Actinobacillus pleuropneumoniae serotype 1. Journal of Veterinary Diagnostic Investigation, 5, 279–282.
- BOSSÉ, J.T., FRIENDSHIP, R., ROSENDAL, S. & FENWICK, B.W., 1993. Development and evaluation of a mixed-antigen ELISA for serodiagnosis of Actinobacillus pleuropneumoniae serotypes 1, 5, and 7 infections in commercial swine herds. Journal of Veterinary Diagnostic Investigation, 5, 359–362.
- BRANDRETH, S.R. & SMITH, I.M., 1985. Prevalence of pig herds affected by pleuropneumonia associated with Haemophilus pleuropneumoniae in eastern England. The Veterinary Record, 117, 143–147.
- CHIERS, K., HAESEBROUCK, F., VAN OVERBEKE, I., CHARLIER, G. & DUCATELLE, R., 1998. In vivo interactions of Actinobacillus pleuropneumoniae with tonsils of pigs. Proceedings of the 15th IPVS Congress, Birmingham, England, 5–9 July 1998, 2, 161.
- CRUIJSEN, T., VAN LEENGOED, L.A.M.G., KAMP, E.M., BARTELSE, A., KOREVAAR, A., VERHEIJDEN, J.H.M., 1995. Susceptibility to Actinobacillus pleuropneumoniae infection in pigs from an endemically infected herd is related to the presence of toxin-neutralizing antibodies. Veterinary Microbiology, 47, 219–228.
- DESROSIERS, R., 1998. Control of bacterial respiratory diseases.Proceedings of the 15th IPVS Congress, Birmingham, England, 5–9 July 1998, 1, 21–25.
- DESROSIERS, R., MITTAL, K.R. & MALO, R., 1984. Porcine pleuropneumonia associated with Haemophilus pleuropneumoniae serotype 3 in Quebec. The Veterinary Record, 115, 628–629.
- DUFF, J.P., SCOTT, W.A., WILKES, M.K. & HUNT, B., 1996. Otitis in a weaned pig: A new pathological role for Actinobacillus (Haemophilus) pleuromoniae. The Veterinary Record, 139, 561–563.
- DUNGWORTH, D.L., 1993. The respiratory system. In: Jubb, K.V.F., Kennedy, P.C. & Palmer, N., (eds). Pathology of Domestic Animals. 4th edn. San Diego, New York, Boston, London, Sydney, Tokyo, Toronto: Academic Press Inc.
- FENWICK, B. & HENRY, S., 1994. Porcine pleuropneumonia. Journal of the American Veterinary Medical Association, 204, 1334–1340.
- FRANK, R.K., CHENGAPPA, M.M., OBERST, R.D., HENNESSY, K.J., HENRY, S.C. & FENWICK, B., 1992. Pleuropneumonia caused by Actinobacillus pleuropneumoniae biotype 2 in growing and finishing pigs. Journal of Veterinary Diagnostic Investigation, 4, 270–278.
- FURESZ, S.E., MALLARD, B.A., BOSSE, J.T, ROSENDAL, S., WILKIE, B.N. & MCINNES, J.I., 1997. Antibody- and cell-mediated immune responses of Actinobacillus pleuropneumoniae-infected and bacterin-vaccinated pigs. Infection and Immunity, 65, 358–365.
- GRAM, T. & AHRENS, P., 1998. Improved diagnostic PCR assay for Actinobacillus pleuropneumoniae based on the nucleotide sequence of an outer membrane lipoprotein. Journal of Clinical Microbiology, 36, 443–448.
- GROMKOVA, R. & KOORNHOF, H., 1990. Naturally occurring NAD-independent Haemophilus parainfluenzae. Journal of General Microbiology, 136, 1031–1035.
- GUTIERREZ, C.B., RODGRIGUEZ BARBOSA, J.I., TASCON, R.I., COSTA, L.I., RIERA, P. & RODRIGUEZ FERRI, E.F., 1995. Serological characterisation and antimicrobial susceptibility of Actinobacillus pleuropneumoniae strains isolated from pigs in Spain. The Veterinary Record, 137, 62–64.
- GUTIERREZ, C.B., PIRIZ, S., VADILLO, S. & RODRIGUEZ FERRI, E.F., 1993. In vitro susceptibility of Actinobacillus pleuropneumoniae strains to 42 antimicrobial agents. American Journal of Veterinary Research, 54, 546–550.
- GUTIERREZ, C.B., TASCON, R.I., VAZQUEZ, J.A. & RODRIGUEZ FERRI, E.F., 1991. Cross-reactivity between Actinobacillus pleuropneumoniae serotypes comparing different antigens and serological tests. Research in Veterinary Science, 50, 308–310.
- HABRUN, B., FREY, J., BILIC, V., NICOLET, J. & HUMSKI, A., 1998. Prevalence of serotypes and tosin types of Actinobacillus pleuropneumoniae in pigs in Croatia. The Veterinary Record, 143, 255–256.
- HAESEBROUCK, F., CHIERS, K., VAN OVERBEKE, I. & DUCATELLE, R., 1997. Actinobacillus pleuropneumoniae infections in pigs: The role of virulence factors in pathogenesis and protection. Veterinary Microbiology, 58, 239–249.
- HENRY, S.C., 1986. Evaluating the alternative therapies for swine respiratory disease. Food Animal Practice/Veterinary Medicine, 81, 763–771.
- HENTON, M.M., 1999. Onderstepoort Veterinary Institute, Onderstepoort. Unpublished data.
- hoffman, l.j., 1989. Actinobacillus (Haemophilus) pleuropneumoniae: Use of coaggulation and complement fixation to determine the relationship between presence of organism and antibody titre in slaughterhouse pigs. Journal of Veterinary Diagnostic Investigation, 1, 12–15.
- HUANG, H.S., POTTER, A.A., CAMPOS, M., LEIGHTON, F.A., WILLSON, P.J. & YATES, W.D.B., 1998. Pathogenesis of porcine Actinobacillus pleuropneumonia: Part I. Effects of surface components of Actinobacillus pleuropneumoniae in vitro and in vivo. Canadian Journal of Veterinary Research, 62, 93–101.
- IBARGOYEN, G.S., PERFUMO, C.J., MASSONE, A.R., MARTIN, A.A. & GRIMENO, E.J., 1989. The use of immunoperoxidase techniques for the identification of Actinobacillus pleuropneumoniae in tissue sections. Israel Journal of Veterinary Medicine, 45, 18–20.
- INZANA, T.J., 1990. Capsules and virulence in the HAP group of bacteria. Canadian Journal of Veterinary Research, 54, 522–529.
- INZANA, T.J., 1995. Simplified procedure for preparation of sensitized latex particles to detect capsular polysaccharides: Application to typing and diagnosis of Actinobacillus pleuropneumoniae. Journal of Clinical Microbiology, 33, 2297–2303.
- JACOBSEN, M.J., NIELSEN, J.P. & NIELSEN, R., 1996. Comparison of virulence of different Actinobacillus pleuropneumoniae serotypes and biotypes using an aerosol infection model. Veterinary Microbiology, 49, 159–168.
- JENSEN, T.K., HAGEDORN-OLSEN, T., RIISING, H.J., THIELSEN, S. & NIELSEN, R., 1998. Osteomyelitis and arthritis caused by Actinobacillus pleuropneumoniae type 2. Pathological description. Proceedins of the 15th IPVS Congress, Birmingham, England, 5–9 July 1998, 3, 385.
- KILIAN, M. & BIBERSTEIN, E.L., 1984. Genus II. Haemophilus. In: KRIEF, N.R. & HOLT, J.G., (eds). Bergey’s Manual of Systematic Bacteriology. Vol. I. Baltimore, London: Williams and Wilkins.
- KUME, K., NAGANO, I. & NAKAI, T., 1986. Bacteriological, serological and pathological examinations of Haemophilus pleuropneumoniae infection in 200 slaughtered pigs. Japanese Journal of Veterinary Science, 48, 965–970.
- LACOUTURE, S., MITTAL, K.R., JACQUES, M., GOTTSCHALK, M., 1997. Serotyping Actinobacillus pleuropneumoniae by the use of monoclonal antibodies. Journal of Veterinary Diagnostic Investigation, 9, 337–341.
- LEVINTHAL, W., 1918. Bakteriologische und serologische influenzastudien. Zeitschrift für Hygiene und Infektionskrankheiten, 86, 1.
- LEWIS, D.H. & SCHWARTZ, W.L., 1987. Haemophilus pleuropneumoniae in swine. Compendium Food Animal, 9, 7–12.
- LIDA, J., SMITH, I.M. & NICOLET, J., 1990. Use of monoclonal antibodies for classifying Actinobacillus (Haemophilus) pleuropneumoniae. Research in Veterinary Science, 49, 8–13.
- LO, T.M., WARD C.K. & INZANA, T.J., 1998. Detection and identification of Actinobacillus pleuropneumoniae serotype 5 by multiplex PCR. Journal of Clinical Microbiology, 36, 1704–1710.
- LOFTAGER, M.-K., ERIKSEN, L., AASTED, B. & NIELSEN, R., 1993. Protective immunity following immunisation of pigs with aerosol of Actinobacillus pleuropneumoniae serotype 2. Research in Veterinary Science, 55, 281–286.
- MCDOWELL, S.W.J. & BALL, H.J., 1994. Serotypes of Actinobacillus pleuropneumoniae isolated in the British Isles. The Veterinary Record, 134, 522–523.
- MIN, K. & CHAE, C., 1998. Detection and distribution of DNA of Actinobacillus pleuropneumoniae in the lungs of naturally infected pigs by in situ hybridization. Journal of Comparative Pathology, 119, 169– 175.
- MITTAL, K.R., 1990. Cross-reactions between Actinobacillus (Haemophilus) pleuropneumoniae strains of serotypes 1 and 9. Journal of Clinical Microbiology, 28, 535–539.
- MITTAL, K.R., HIGGINS, R. & LARIVIERE, S., 1988. Serologic studies of Actinobacillus (Haemophilus) pleuropneumoniae strains of serotype 3 and their antigenic relationship with other Actinobacillus pleuropneumoniae serotypes in swine. American Journal of Veterinary Research, 49, 152–155.
- MITTAL, K.R., HIGGINS, R., LARIVIERE, S. & MARTINEAU, G., 1985. Use of coagglutination test for direct detection and serotyping of Haemophilus pleuropneumoniae. Compendium on Swine Haemophilus Pleuropneumonia, 28–33.
- MITTAL, K.R., HIGGINS, R., LARIVIERE, S. & MARTINEAU, G.P., 1987. Effect of heat treatment on the surface antigens of Haemophilus pleuropneumoniae. The Veterinary Record, 120, 62–65.
- MOLLER, K. & KILIAN, M., 1990. V factor dependent members of the family Pasteurellaceae in the porcine upper respiratory tract. Journal of Clinical Microbiology, 28, 2711–2716.
- MOROZUMI, T. & HIRAMUNE, T., 1982. Effect of temperature on the survival of Haemophilus parasuis in physiological saline. National Institute of Animal Health. (Tokyo), 22, 90–91.
- MYLREA, P.J., FRASER, G., MACQUEEN, P. & LAMBOURNE, D.A., 1974. Pleuropneumonia in pigs caused by Haemophilus parahaemolyticus. Australian Veterinary Journal, 50, 255–259.
- NARITA, M., KAWASHIMA, K., MOROZUMI, T. & TAKASHIMA, H., 1995. Effect of physical defenses of the respiratory tract on the development of pneumonia in pigs inoculated endobronchially with Actinobacillus pleuropneumoniae. Journal of Veterinary Medical Science, 57, 839–844.
- NICOLET, J., 1985. Haemophilus pleuropneumoniae—Bacteriology and epidemiology. Compendium on Swine Haemophilus Pleuropneumonia, 7–11.
- NICOLET, J., 1992. Actinobacillus pleuropneumoniae. In: LEMAN, A.D., STRAW, B., MENGELING, W.L., D’ALLAIRE, S., TAYLOR, D.J., (eds). Diseases of Swine. 7th edn. Ames, Iowa: Iowa State University Press.
- NICOLET, J., 1988. Taxonomy and serology identification of Actinobacillus pleuropneumoniae. Canadian Veterinary Journal, 29, 578–579.
- NIELSEN, R., 1982. Haemophilus pleuropneumoniae infection in pigs. Thesis, Veterinaer-og Landbohojskoles, Copenhagen, Denmark.
- NIELSEN, R., 1985. Haemophilus pleuropneumoniae diagnosis, immunity and control. Compendium on Swine Haemophilus Pleuropneumonia, 18–22.
- NIELSEN, R., 1988. Seroepidemiology of Actinobacillus pleuropneumoniae. Canadian Veterinary Journal, 29, 580–582.
- OLANDER, H.J., 1985. The pathology of Haemophilus pleuropneumoniae infection of swine. Compendium on Swine Haemophilus Pleuropneumonia, 12–17.
- PATTISON, I.H., HOWELL, D.C. & ELLIOTT, J., 1957. A Haemophilus-like organism isolated from pig lung and the associated pneumonic lesion. Journal of Comparative Pathology, 67, 320–329.
- POHL, S., BERSTSCHINGER, H.U., FREDERIKSEN, W., MANNHEIM, W., 1983. Transfer of Haemophilus pleuropneumoniae and the Pasteurella haemolytica-like organism causing porcine necrotic pleuropneumonia to the genus Actinobacillus (Actinobacillus) pleuropneumoniae comb. nov.) on the basis of phenotypic and deoxyribonucleic acid relatedness. International Journal of Systematic Bacteriology, 33, 510–514.
- POL, J.M.A., VAN LEENGOED, L.A.M.G., STOCKHOFE, N., KOK, G. & WENSVOORT, G., 1997. Dual infections of PRRSV/influenza or PRRSV/Actinobacillus pleuropneumoniae in the respiratory tract. Veterinary Microbiology, 55, 259–264.
- RAEMDONCK, D.L., TANNER, A.C., TOLLING, S.T. & MICHENER, S.L., 1994. Antimicrobial susceptibility of Actinobacillus pleuropneumoniae, Pasteurella multocida and Salmonella choleraesuis isolates from pigs. The Veterinary Record, 134, 5–7.
- RIOUX, S., GIRARD, C., DUBREUIL, J.D. & JACQUES, M., 1998. Evaluation of the protective efficacy of Actinobacillus pleuropneumoniae serotype 1 detoxified lipopolysaccharides or O-polysaccharide-protein conjugate in pigs. Research in Veterinary Science, 65, 165–167.
- ROHRBACH, B.W., HALL, R.F. & HITCHCOCK, J.P., 1993. Effect of subclinical infection with Actinobacillus pleuropneumoniae in comingled feeder swine. Journal of the American Veterinary Medical Association, 202, 1095–1098.
- SAKANO, T., SHIBATA, I., SAMEGAI, Y, TANEDA, A., OKADA, M., IRISAWA, T. & SATO, S., 1993. Experimental pneumonia of pigs infected with Aujeszky’s disease virus and Actinobacillus pleuropneumoniae. Journal of Veterinary Medical Science, 55, 575–579.
- SCHULTZ, R.A., 1985. Haemophilus pleuropneumoniae of swine: Prevalence, treatment, control and prevention. Compendium on Swine Haemophilus Pleuropneumonia, 34–38.
- SEBUNYA, T.N.K. & SAUNDERS, J.R., 1983. Haemophilus pleuropneumoniae infection in swine: A review. Journal of the American Veterinary Medical Association, 182, 1331–1337.
- SIDIBÉ, M., MESSIER, S., LARIVIERE, S., GOTTSCHALK, M. & MITTAL, K.R., 1993. Detection of Actinobacillus pleuropneumoniae in the porcine upper respiratory tract as a complement to serological tests. Canadian Journal of Veterinary Research, 57, 204–208.
- STINE, D.L., FEDORKA-CRAY, P.J., HUETHER, M.J., GENTRY, M.J. & ANDERSON, G.A., 1994. Comparison of serum responses in swine after vaccination and challenge exposure with Actinobacillus pleuropneumoniae serotype 1. American Journal of Veterinary Research, 55, 1238–1243.
- STRAW, B., 1986. A look at the factors that contribute to the development of swine pneumonia. Food Animal Practice/Veterinary Medicine, 81, 747–756.
- TARASIUK, K., PEJSAK, Z., PALKA, E. & BLASZCZYK, B., 1991. Acute form of pleuropneumonia in pigs caused by Actinobacillus pleuropneumoniae serotype 9. Medycyna Weterynaryjna, 47, 348–350.
- TARIGAN, S., SLOCOMBE, R.F., BROWNING, G.F. & KIMPTON, W., 1994. Functional and structural changes of porcine alveolar macrophages induced by sublytic doses of a heat labile, haemolytic, cytotoxic substance produced by Actinobacillus pleuropneumoniae. American Journal of Veterinary Research,55, 1548–1557.
- THIELSEN, S., HAGEDORN-OLSEN, T., JENSEN, T.K., NIELSEN, R. & RIISING, H.J., 1998. An outbreak of Actinobacillus pleuropneumoniae type 2, characterized by osteomyelitis, arthritis and pleuropneumonia. Proceedings of the 15th IPVS Congress, Birmingham, England, 5–9 July 1998, 3, 384.
- THOMAS, P., 1984. The influence of housing design and some management systems on the health of the growing pig particularly in relation to pneumonia. Commonwealth Agricultural Bureaux: Pig News and Information, 5, 343–349.
- TORREMORELL, M., PIJOAN, C., JANNI, K., WALKER, R. & JOO, H.S., 1997. Airborne transmission of Actinobacillus pleuropneumoniae and porcine reproductive and respiratory syndrome virus in nursery pigs. American Journal of Veterinary Research, 58, 828–832.
- TUBBS, R.C., 1988. Managing the swine herd that’s been infected with Haemophilus pleuropneumoniae. Food Animal Practice/Veterinary Medicine, 83, 220–229.
- TURK, J.R., FALES, W.H., MADDOX, C.W., RAMOS, J.A., FISCHER, J.R., JOHNSON, G.C., KREEGER, J.M., MILLER, M.A., PACE, L.W., TURNQUIST, S.E. & GOSSER, H.S., 1993. Pleuropneumonia in Missouri swine. Journal of Veterinary Diagnostic Investigation, 5, 101–103.
- UDEZE, F.A. & KADIS, S., 1992. Effects of Actinobacillus pleuropneumoniae hemolysin on porcine neutrophil function. Infection and Immunity, 60, 1558–1567.
- UDEZE, F.A., LATIMER, K.S. & KADIS, S., 1987. Role of Haemophilus pleuropneumoniae lipopolysaccharide endotoxin in the pathogenesis of porcine Haemophilus pleuropneumoniae. American Journal of Veterinary Research, 48, 768–773.
- WILSON, P.J., FALK, G. & KLASHINSKY, S., 1987. Detection of Actinobacillus pleuropneumoniae infection in pigs. Canadian Veterinary Journal, 28, 111–116.
- WILSON, P.J., SCHIPPER, C. & MORGAN, E.D., 1988. The use of an enzyme-linked immunosorbent assay for diagnosis of Actinobacillus pleuropneumoniae infection in pigs. Canadian Veterinary Journal, 29, 583–585.
- ZUMPT, G.F., 1999. Box 2515, Randburg, 2125. Personal communication.




