- Infectious Diseases of Livestock
- Part 3
- Strangles
- GENERAL INTRODUCTION: SPIROCHAETES
- Swine dysentery
- Borrelia theileri infection
- Borrelia suilla infection
- Lyme disease in livestock
- Leptospirosis
- GENERAL INTRODUCTION: AEROBIC ⁄ MICRO-AEROPHILIC, MOTILE, HELICAL ⁄ VIBROID GRAM-NEGATIVE BACTERIA
- Genital campylobacteriosis in cattle
- Proliferative enteropathies of pigs
- Campylobacter jejuni infection
- GENERAL INTRODUCTION: GRAM-NEGATIVE AEROBIC OR CAPNOPHILIC RODS AND COCCI
- Moraxella spp. infections
- Bordetella bronchiseptica infections
- Pseudomonas spp. infections
- Glanders
- Melioidosis
- Brucella spp. infections
- Bovine brucellosis
- Brucella ovis infection
- Brucella melitensis infection
- Brucella suis infection
- Brucella infections in terrestrial wildlife
- GENERAL INTRODUCTION: FACULTATIVELY ANAEROBIC GRAM NEGATIVE RODS
- Klebsiella spp. infections
- Escherichia coli infections
- Salmonella spp. infections
- Bovine salmonellosis
- Ovine and caprine salmonellosis
- Porcine salmonellosis
- Equine salmonellosis
- Yersinia spp. infections
- Haemophilus and Histophilus spp. infections
- Haemophilus parasuis infection
- Histophilus somni disease complex in cattle
- Actinobacillus spp. infections
- Actinobacillus equuli infections
- Gram-negative pleomorphic infections: Actinobacillus seminis, Histophilus ovis and Histophilus somni
- Porcine pleuropneumonia
- Actinobacillus suis infections
- Pasteurella and Mannheimia spp. infections
- Pneumonic mannheimiosis and pasteurellosis of cattle
- Haemorrhagic septicaemia
- Pasteurellosis in sheep and goats
- Porcine pasteurellosis
- Progressive atrophic rhinitis
- GENERAL INTRODUCTION: ANAEROBIC GRAM-NEGATIVE, IRREGULAR RODS
- Fusobacterium necrophorum, Dichelobacter (Bacteroides) nodosus and Bacteroides spp. infections
- GENERAL INTRODUCTION: GRAM-POSITIVE COCCI
- Staphylococcus spp. infections
- Staphylococcus aureus infections
- Exudative epidermitis
- Other Staphylococcus spp. infections
- Streptococcus spp. infections
- Strangles
- Streptococcus suis infections
- Streptococcus porcinus infections
- Other Streptococcus spp. infections
- GENERAL INTRODUCTION: ENDOSPORE-FORMING GRAM-POSITIVE RODS AND COCCI
- Anthrax
- Clostridium perfringens group infections
- Clostridium perfringens type A infections
- Clostridium perfringens type B infections
- Clostridium perfringens type C infections
- Clostridium perfringens type D infections
- Malignant oedema⁄gas gangrene group of Clostridium spp.
- Clostridium chauvoei infections
- Clostridium novyi infections
- Clostridium septicum infections
- Other clostridial infections
- Tetanus
- Botulism
- GENERAL INTRODUCTION: REGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Listeriosis
- Erysipelothrix rhusiopathiae infections
- GENERAL INTRODUCTION: IRREGULAR, NON-SPORING, GRAM-POSITIVE RODS
- Corynebacterium pseudotuberculosis infections
- Corynebacterium renale group infections
- Bolo disease
- Actinomyces bovis infections
- Trueperella pyogenes infections
- Actinobaculum suis infections
- Actinomyces hyovaginalis infections
- GENERAL INTRODUCTION: MYCOBACTERIA
- Tuberculosis
- Paratuberculosis
- GENERAL INTRODUCTION: ACTINOMYCETES
- Nocardiosis
- Rhodococcus equi infections
- Dermatophilosis
- GENERAL INTRODUCTION: MOLLICUTES
- Contagious bovine pleuropneumonia
- Contagious caprine pleuropneumonia
- Mycoplasmal pneumonia of pigs
- Mycoplasmal polyserositis and arthritis of pigs
- Mycoplasmal arthritis of pigs
- Bovine genital mycoplasmosis
- Neurotoxin-producing group of Clostridium spp.
- Contagious equine metritis
- Tyzzer's disease
- MYCOTIC AND ALGAL DISEASES: Mycoses
- MYCOTIC AND ALGAL DISEASES: Pneumocystosis
- MYCOTIC AND ALGAL DISEASES: Protothecosis and other algal diseases
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Epivag
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ulcerative balanoposthitis and vulvovaginitis of sheep
- DISEASE COMPLEXES / UNKNOWN AETIOLOGY: Ill thrift
- Eperythrozoonosis
- Bovine haemobartonellosis
Strangles
This content is distributed under the following licence: Attribution-NonCommercial CC BY-NC  View Creative Commons Licence details here
View Creative Commons Licence details here
Strangles
Previous Author: J F TIMONEY
Current Authors:
A S WALLER - Head of Bacteriology, BSc, PhD, Animal Health Trust, Lanwades Park, Kentford, Newmarket, Suffolk, CB8 7UU, United Kingdom
![]()
Introduction
Strangles is an acute contagious disease of horses, mules and donkeys characterized by fever, acute mucopurulent inflammation of the upper respiratory tract, purulent lymphadenitis and abscessation of the submandibular and retropharyngeal lymph nodes.60 The disease was first described by Jordanus Rufus in 125152 and the causative agent, Streptococcus equi, was identified in 1888.53 However, genetic analysis dates the common ancestor of contemporary strains of S. equi to the late 19th or early 20th Century.26 This period of history was blighted by a series of global conflicts, in which the horse played vital roles. The increased breeding and global transport of horses to replace those killed on the battlefields is thought to have facilitated a population replacement of S. equi, resulting in the emergence and dissemination of the ‘fittest’ strain to horse populations around the world.67 The modern day transport of S. equi around the world is now known to be facilitated by the ability of S. equi to persist in the guttural pouches or sinuses of a proportion of carrier horses following their recovery from acute disease.23, 45 The transition of S. equi between acute and persistent forms of infection is critical to its success as a pathogen and breaking this cycle through improved biosecurity, diagnostics and vaccines is essential to reducing the global prevalence and impact of strangles.
Strangles is endemic throughout the world with outbreaks in Europe, Australia, New Zealand, India, Malaysia, South Africa, Japan, and North and South America. Indeed, only Iceland remains free of strangles, a situation that is likely due to virtually no importation of horses over the last 1,000 years.11 It is estimated that over 600 outbreaks of strangles occur in the UK each year.30 Information derived from reports submitted annually by 20 countries to the International Collating Centre of the Animal Health Trust, Newmarket, England, indicates that strangles ranks with equine influenza and herpesvirus abortion as one of the three most significant equine infectious diseases.
The outbreaks in 1998 of strangles in the Western Cape Province of South Africa occurred after an interval of 20 years’ freedom from the disease and owe their origin to the introduction of S. equi in breeding stock imported from Australia. Previous outbreaks occurred in Thoroughbred mares and foals during the period November 1977 to February 1978, after the mares had visited the Western Cape for service during the 1977 breeding season. Many contracted the disease during the visit before returning to their home stud farms in the Eastern Cape, Karoo and KwaZulu-Natal.
Theiler58 reported on the occurrence in South Africa of sporadic cases and epidemics in the earlier part of the 1900s and considered that aged horses were to a very great extent immune as they had ‘passed through the disease at an earlier age — very few horses escaping it altogether whilst young’. This was before the major decline in equine populations took place throughout the world. During World War II thousands of horses and mules were shipped from South Africa to India to be used as pack animals in the Burma Campaign. Many of these animals were congregated at a military base camp in Pinetown before shipment from Durban harbour. Periodic outbreaks of strangles occurred in this camp.
Aetiology
Streptococcus equi has evolved from an ancestral strain of the opportunistic pathogen S. zooepidemicus through a process of gene loss and gain.29, 33, 71 Individual cells are ovoid or spherical, 0.6 to 1.0 µm in diameter, Gram-positive and may form long chains in pus and in recently infected lymph nodes. Excellent aerobic and anaerobic growth occurs in Todd Hewitt broth with 0.2 per cent yeast extract, in chemically defined medium64 and in common laboratory media supplemented with serum. The organism produces the β-haemolytic toxin streptolysin S18 and carries a Lancefield Group C carbohydrate typing antigen.
A hyaluronic acid capsule is produced by most strains and is most evident in logarithmic phase cultures. The accumulation of a hyaluronic acid capsule is likely due to a mutation in the genome-encoded hyaluronate lyase gene, which is present in all strains of S. equi.29 The capsule shields S. equi from the host immune response3 and its production in some persistent strains is further enhanced by amplification of the biosynthetic has locus, whilst other persistent strains contain deletions, nonsense mutations and non-synonymous mutations in the has locus that can eliminate production of hyaluronic acid.26 Such variability may reflect an increased need for S. equi to evade the immune response of recently recovered animals, but suggests that the production of hyaluronic acid in the guttural pouch is unfavourable in the longer term. The lack of has mutations in populations of S. equi recovered from acute cases of strangles suggests that the decay of the has locus may be an evolutionary dead-end for S. equi and that such strains have a reduced capacity to transmit to naïve animals and cause disease.
The genomes of all strains of S. equi, but no strains of S. zooepidemicus, contain ICESe2, an integrative conjugative element, which encodes the non-ribosomal peptide biosynthesis system (NRPS) that produces equibactin.29 The equibactin NRPS has structural similarities with the yersiniabactin NRPS of Yersinia pestis, the causative agent of bubonic plague.27 The production of yersiniabactin, an iron-binding siderophore, is essential to the disease-causing ability of Y. pestis.7 Similarly, equibactin production enhanced the ability of S. equi to acquire iron27 and was essential for the full virulence of S. equi in ponies.26 Some strains of S. equi that persistently infect the guttural pouches of carrier horses may contain deletions in the equibactin locus that render it non-functional.26 However, to date, all strains recovered from acutely affected horses contain a complete equibactin locus.26 These data provide support for the hypothesis that the genetic acquisition of ICESe2 was the speciation event in the evolution of S. equi from S. zooepidemicus.29
The genomes of S. equi contain multiple prophage elements,26, 29 possibly acquired as a consequence of a deletion in the CRISPR-cas29, 69 locus that would normally confer resistance to prophage acquisition.11 The φSeq4 prophage of S. equi strain 4047 (Se4047) encodes a hyaluronan-specific hyaluronate lyase, which is produced during infection of horses.38 φSeq3 and φSeq4 of Se4047 together encode the superantigens SeeH, SeeI, SeeL and SeeM, which are secreted into culture media in vitro 4, 46 and the local environment during infection of the horse,41 stimulating strong pro-inflammatory responses that likely contribute to abscess formation.29, 46 Streptococcus equi strains produce two phospholipase A2 toxins, SlaA and SlaB, which are encoded in φSeq2 of Se4047 and a prophage remnant in the genome of all S. equi and S. zooepidemicus strains.29 Phospholipase A2 toxins cleave phospholipid molecules, contributing to the production of leukotrienes that modulate inflammation.40 Some S. equi strains encode multiple copies of SlaA,26 the consequences of which are currently unknown. The Se4047 φSeq1 encodes no cargo elements (superantigens or phospholipase A2 toxins).29 This prophage element is diverse between different strains of S. equi and evidence of prophage transmission between co-circulating strains of S. equi is evident in whole genome sequencing data.26 Such plasticity in the array of mobile genetic elements possessed by different strains of S. equi may influence their virulence and ability to transmit to other horses.
Streptococcus equi strains encode 29 sortase-processed surface proteins, but lack functional homologues of several S. zooepidemicus cell surface proteins including the FimII, FimIII and FimIV putative pilus loci.8, 29 Pili play an important role in the adherence of streptococci to host tissues1, 47 and the reduced complement of pili and other sortase-processed proteins on the surface of S. equi may limit its ability to bind to an array of host tissues and to occupy diverse pathogenic niches, providing one explanation for the restriction of S. equi infection to horses.29 All strains of S. equi retain the FimI locus, whose accessory pilin protein, CNE, shares homology to CNA of S. aureus and has been similarly shown to bind collagen.36 This pilus locus is present in the genomes of every strain of S. equi (and S. zooepidemicus) examined to date11, 26, 29, 55 and is likely to play an important role in general adhesion to host tissues.55 In support of the importance of FimI, a multicomponent subunit vaccine containing recombinant CNE conferred protection against S. equi infection of Welsh mountain ponies.24
The most variable gene within the core genome of S. equi encodes an antiphagocytic sortase-processed M-like cell surface protein, SeM.12, 13 Variation in SeM is restricted to the N-terminal region, the DNA sequence of which can be used to differentiate strain types.2, 34 The gene encoding SeM may be truncated in isolates recovered from persistently infected horses.14, 26, 34 Furthermore, some strains of S. equi accumulate non-synonymous SeM mutations as they establish persistent infection.26, 34 These data suggest that non-synonymous SeM variants may be more able to evade immune responses targeting this protein that are produced by convalescent horses, facilitating persistence, shedding and onward transmission. The lack of SeM deletions in strains causing acute strangles suggests that SeM plays an important role in the ability of S. equi to cause strangles and that decay of SeM is another evolutionary dead-end. Full length SeM binds fibrinogen, IgG4 and IgG7 sub-classes.37, 42 Fibrinogen binding masks C3b-binding sites on the bacterial surface, reducing the rate of phagocytosis.13, 37, 42
Epidemiology
Strangles occurs in animals of all ages, but is more common in those less than two years old. While the majority of animals that recover from an initial attack of strangles are subsequently immune, some may contract the disease for a second or even a third time.63 Immune mares confer passive immunity to their foals, which protects the foals until the age of three months.21 However, infection may be transmitted by diseased foals to their dams during suckling, with the subsequent development of purulent mastitis. Contamination of surgical and other wounds may also occur, but in these cases typical strangles does not occur: the infection remains localized at the site and its regional lymph node. Adult animals that have grown up in relative isolation remain fully susceptible and may become severely ill following exposure to S. equi.
Streptococcus equi is an obligate parasite and requires equids for its survival and interepidemic maintenance.60 Horses suffering acute strangles shed large quantities of S. equi into the environment. The disease is highly contagious, transmission occurring via the oral and nasal routes, the former being more common.60 Contaminated feed, water, bedding, stables and stable utensils, including tack or harnesses, are important in the spread of the infection.60 Streptococcus equi may survive for several weeks in water troughs,32 but dies quickly in soil and on pasture. Contaminated surfaces of stables do not remain infective for more than a few days. Survival requires moisture, protection from sunlight and absence of environmental microbial contaminants. Therefore, the environment is not a significant reservoir of infection, but plays an important role in disease transmission from one horse to another.
A proportion of horses that recover from strangles remain persistently infected with S. equi, usually harbouring the bacteria within their guttural pouches or sinus. Streptococcus equi can be intermittently shed from these persistently infected, but healthy carrier horses for several years, providing a reservoir of infection that facilitates interepidemic maintenance of S. equi and its introduction to premises previously free of the disease.23, 45 The identification and treatment of carriers to eliminate S. equi is critical if future outbreaks of strangles are to be prevented.
On farms and in stables which have a high population density of horses and a rapid turnover of animals, there is an increased risk of infection. In a survey of 179 stud farms in Australia during the period 1985 to 1988 it was found that the risk of strangles increased progressively and dramatically with the total horse population.72 Stud farms with a population of more than 100 horses had 26.2 times greater risk than those with less than 15 horses.
Stressful situations, particularly those caused by transportation, very cold or hot weather and overcrowding, enhance susceptibility and transmission. As infection and shedding of S. equi progress in a group, the burden of challenge increases and so animals with moderate levels of protective immunity may succumb. It is therefore very important to isolate strangles cases during the acute and immediate convalescent phases until shedding ceases. It is also important to identify and treat persistently infected carriers once horses recover and before they can transmit the infection to new premises.
Pathogenesis, clinical signs and pathology
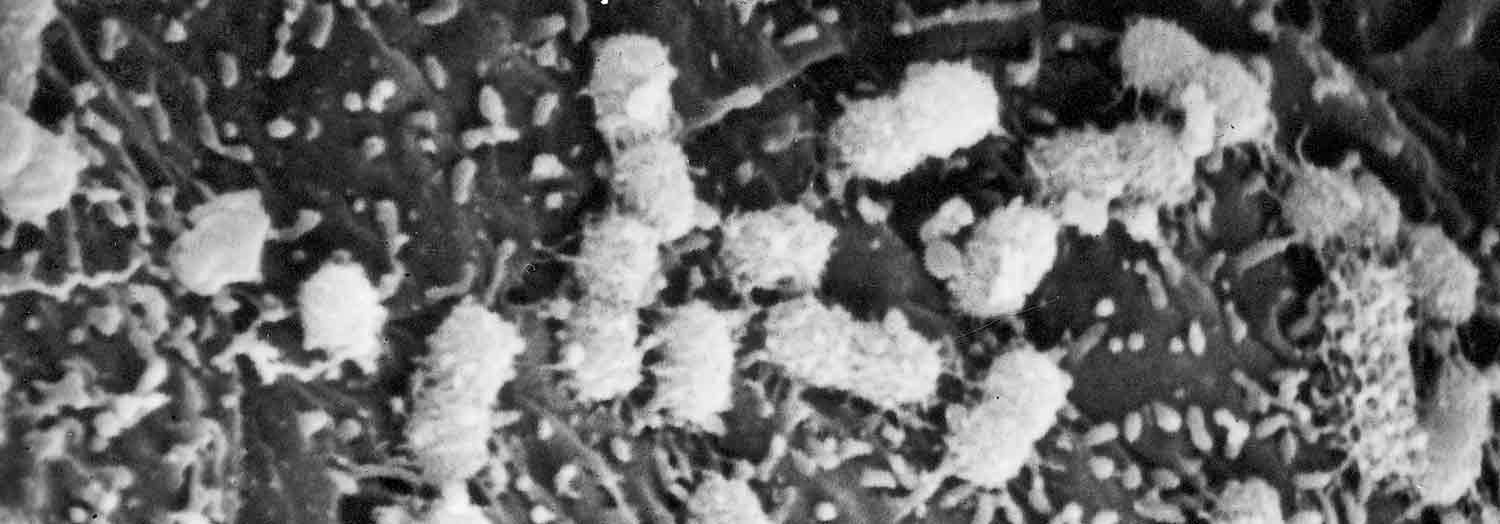
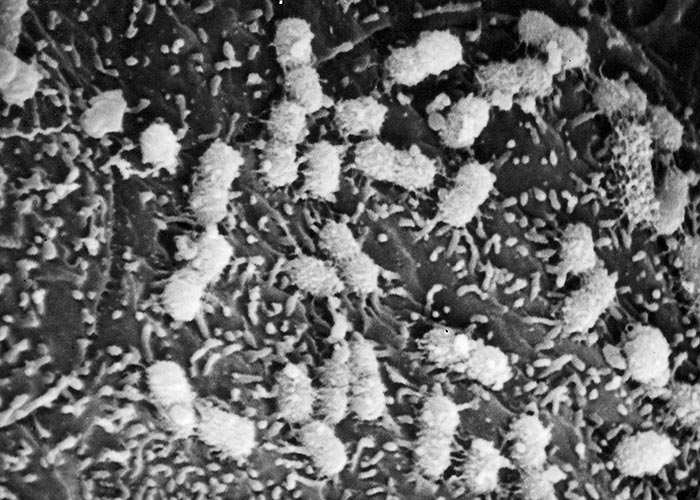
Streptococcus equi enters a new host via the oral and respiratory routes. Adherence appears to primarily involve tonsillar crypt epithelial cells and the epithelium of the ventral surface of the soft palate.62 Scanning electron microscopy studies have confirmed that S. equi binds to tonsillar crypt epithelium and is not detectable by this technique on the surface of other areas of the mouth and nasopharynx (Figure 1).
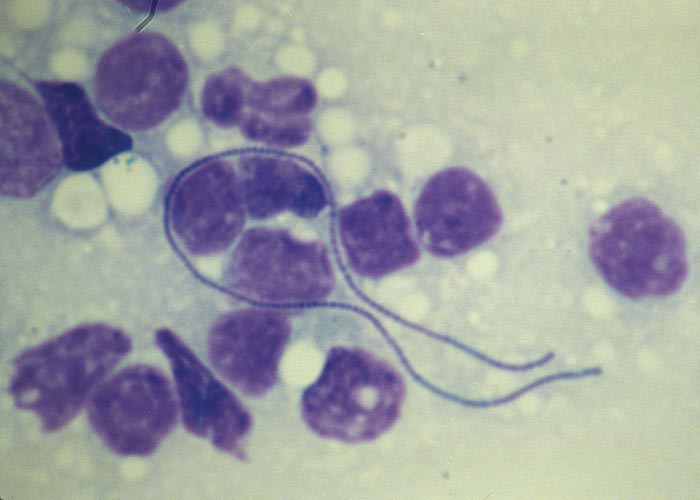
Within hours of experimental infection, S. equi is difficult to detect on the mucosal surface,62 but can be cultured from the regional lymph nodes where it multiplies extracellularly forming long chains (Figure 2). Although interaction of C3 with bacterial peptidoglycan generates complement-derived chemotactic factors that attract large numbers of neutrophils,43 phagocytosis and bacterial killing are poor due to a combination of hyaluronic acid capsule, antiphagocytic SeM and other proteins produced by S. equi.68
As abscesses develop in the lymph nodes, the flow of lymph may be restricted, resulting in the swelling of the submandibular region (‘jugging up’) or occlusion of the airway (‘strangles’) (Figure 3). Although strangles primarily involves airways and associated lymph nodes, metastasis to lymph nodes of the thorax and abdomen and to the brain may occur.17

Strangles spreads very rapidly in a group of susceptible horses mainly via communal water troughs and feeders. Under conditions of stress (heat, cold, crowding, and prolonged rain) the incubation period may be as short as four to five days. However, since not all horses become infected at the same time or with the same dose of S. equi, the apparent incubation period in some horses may be as long as 21 days after exposure. In outbreaks the morbidity varies from 10 to 100 per cent, but the mortality rate is low and ranges from about one to five per cent.56, 57 The course of strangles in mild and uncomplicated cases is seldom longer than two to four weeks and generally terminates in complete recovery.56 However, in some horses, the disease may be protracted and last for several months.57
Three clinical forms are described — typical, atypical (catarrhal) and bastard strangles. The typical disease begins after an incubation period of three to 12 days and is heralded by a sudden sharp rise in rectal temperature to 39 °C and haematological changes, including leukocytosis with leukocyte blood counts up to 30 000/µl, a segmented neutrophil count that may exceed 25 000/µl, and a fibrinogen level of 6.0 mg/dl. These are signs of an acute phase reaction probably mediated by the release of inflammatory cytokines IL-1 and TNFα, triggered by exposure of leukocytes to S. equi. The fever is often accompanied by anorexia and depression and is soon followed by the development of a serous nasal discharge which, during the course of two to three days, becomes mucopurulent, then purulent and, finally, thick and yellow. The discharge is generally bilateral but may be more profuse from one nostril than the other. A soft, moist cough may be present and can usually be elicited by manual compression of the pharynx or larynx. Breathing may be noisy and laboured and large quantities of exudate can be expelled from the nostrils during bouts of coughing, snorting or blowing. The pharyngeal area is painful and the animal stands with its head lowered and extended (Figure 3). The act of swallowing may be impeded. These clinical signs are the result of an acute purulent rhinitis, pharyngitis and, in some cases, laryngitis with hyperaemia and swelling of the mucosa and accumulation of pus in the nasal cavities. Small abscesses may develop in the lymphoid follicles of the soft palate. A catarrhal or purulent conjunctivitis with ocular discharge may be present.
In typical cases of strangles it soon becomes apparent that there is concurrent involvement of the regional lymph nodes draining the nasopharynx, particularly those of the submandibular and retropharyngeal areas, and, in some animals, the submaxillary and parotid regions. Affected nodes are hot, swollen and painful, and are initially firm on palpation for about four to six days after which time they become softer and considerably larger. The covering skin is tense and becomes thin and exudes a serum-like fluid. The severe lymph node enlargement, together with mucosal changes, may impede mastication, swallowing and respiration, and may be so severe as to result in asphyxiation. Finally, after about five to ten days, the abscess or abscesses rupture, discharging large quantities of thick, yellow, creamy pus. Abscesses in the retropharyngeal lymph nodes may rupture externally or internally, i.e. discharge their contents into the pharynx or guttural pouch. Rupture is commonly followed by a rapid decline in the fever and an improvement in the habitus of the animal. Occasionally, small vesicles, ulcers and scabs form in the skin of various parts of the body, particularly on the cheeks, nose, mouth, sides of the neck, and chest.
Streptococcus equi is very sensitive to penicillin and its administration in the early febrile stage before abscess development may be effective in preventing further development of the disease. Treated animals, however, are unlikely to generate protective immune responses and remain susceptible.56 They must be protected against further exposure to S. equi. Antibiotic therapy in the later stages of strangles when abscesses are present will be associated with temporary clinical improvement, but may not eradicate the infection and may even prolong the course of the disease. It is preferable therefore to allow uncomplicated strangles cases to run their course without intervention of antibiotic therapy, which should be reserved for cases with dyspnoea, prolonged high fever, severe lassitude and anorexia. Other antimicrobials that may be used include trimethoprim-sulphonamide, erythromycin, tetracyclines, lincomycin and ampicillin.
In the atypical mild catarrhal form,63 which occurs most commonly in older horses with residual immunity, manifestations of the disease remain confined to a catarrhal inflammation of the upper respiratory tract, generally without regional lymphadenopathy; if the latter does occur, abscesses in the nodes either do not develop or, if they do, often become encapsulated without rupturing.
More severe forms of strangles may result in a fatal outcome.57 They include: spread of the infection to the sinuses with resultant purulent sinusitis; periorbital abscessation; paravertebral abscessation; roaring following recurrent nerve involvement in the inflammatory process; purulent pneumonia as the result of aspiration of pus into the lungs; agalactia in lactating mares; asphyxiation following upper respiratory tract obstruction; myopathy; myocarditis that may cause significant electrocardiographic abnormalities that persist for several months; endocarditis; pyaemia; and purpura haemorrhagica.
Pyaemia may result in the form of strangles known as ‘bastard strangles’, in which S. equi has metastasized to lymph nodes other than those regional to the upper respiratory tract, and to organs, such as the liver, kidneys, lungs, and brain, with resultant abscess formation, as well as to synovial structures of the limbs with purulent arthritis and tenosynovitis. Of the internal organs, the mesenteric and mediastinal lymph nodes are most commonly affected. Although these abscesses may become very large, they rarely rupture, but the infection may spread per continuitatum from them to reach nearby serosal surfaces with the development of purulent peritonitis or pleuritis. Affected horses exhibit loss of weight, intermittent fever, neutrophilia, and a high level of antibody to S. equi. The fever and neutrophilia may be responsive to penicillin administration. Appropriate local treatment, including draining of abscesses may be of benefit.9, 49
Anaemia is a common sequela to strangles and is associated with moderate decreases in haemoglobin concentration, mean packed cell volume, and erythrocyte count that begin during convalescence and persist for some weeks after clinical recovery.25 The onset of the anaemia during convalescence would seem to implicate an immune-mediated mechanism. It is also possible that the effect is due to depression of haematopoiesis by TNFα released during the acute phase reaction.
Muscle infarction in which the typical histopathologic lesion is acute coagulative necrosis with vasculitis can occur in horses with a recent history of strangles.56 The condition is usually fatal and accompanied by severe pain and muscle stiffness, colic and multifocal subcutaneous swelling. Elevated levels of serum creatinine kinase (CK) and aspartate aminotrasferase (AST) may be observed. Multifocal areas of pulmonary haemorrhage and gastrointestinal infarctions are also commonly present. This complication may accompany purpura haemorrhagica.
Chronic active rhabdomyolysis involving the epaxial and gluteal muscles has also been described as a complication of S. equi infection.56 Affected horses may not have overt clinical signs of strangles but show malaise and a rapidly progressive atrophy of the gluteal muscles. Serum aspartate aminotransferase (AST) and CK levels are elevated and muscle biopsy sections are characterized by chronic active rhabdomyolysis with macrophage infiltration, lymphocytic vasculitis and atrophy of fast twitch fibres. The condition is responsive to a combination of penicillin and dexamethasone therapy followed by prednisone for a month.
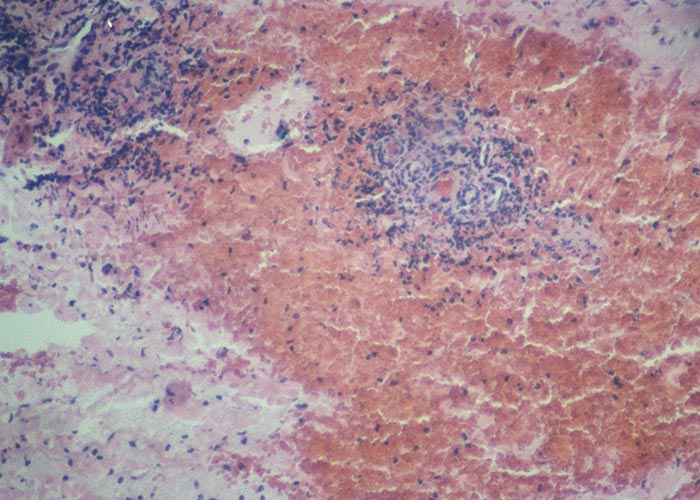
Purpura haemorrhagica, an acute nonthrombocytopenic leukocytoclastic vasculitis, is another serious sequela of strangles. It occurs in a small percentage (≤ per cent) of horses two to four weeks following the acute phase of strangles and is also occasionally observed a week or two following vaccination with the Pinnacle IN live attenuated vaccine.48 Affected horses exhibit oedema of the head, legs and ventral abdomen, and petechiae in the oral and conjunctival mucosae are usually present. Urticarial plaques may appear and exude serum. Skin necrosis with sloughing may then occur. Diarrhoea and colic may be present as a result of ulcerative necrosis of the intestinal mucosa. Oedema of the lungs may cause respiratory distress. Glomerulonephritis associated with proteinuria and azotaemia has also been described. Haematological changes include anaemia with a reduced erythrocyte count, a PCV of about 30 per cent, a haemoglobin level of less than 80mg/ml, aleukocytosis with a shift to the left, and an increased C3 level.10 Platelet counts are in the normal range.10 The primary lesion is a leukocytoclastic vasculitis with necrosis of blood vessel walls and extravasation of erythrocytes (Figure 4). Very high levels of serum antibody to the surface proteins of S. equi and a high C3 level are usually present before, during and after an episode of purpura haemorrhagica.60 Horses that develop the condition are therefore hyper-responsive with respect to antibody production. SeM-IgA immune complexes have been detected in sera, suggesting a resemblance to Schönlein-Henoch’s purpura haemorrhagica in humans.19 The mortality rate is 50 per cent or higher in cases of severe purpura haemorrhagica. The diagnosis of the condition is based on a history of recent exposure to S. equi or S. equi vaccine,48 a very high level of serum antibodies to S. equi, and histopathological evidence of leukocytoclastic vasculitis in biopsy specimens. Horses with purpura haemorrhagica can be treated with dexamethasone and, where infection is active, with antibiotics. Supportive care through the administration of intravenous fluids, hydrotherapy and bandaging may also be of benefit.
Agalactia (in the absence of detectable physical abnormalities in the mammary glands) may be secondary to the high fever, anorexia and depression associated with strangles. Though this complication is not life-threatening, it may become a serious management problem, as alternative sources of milk have to be found for the foals of mares suffering from the condition. Abortion is also a complication in mares affected in late pregnancy.
Signs of septicaemia and polyarthritis commonly occur in foals infected with S. equi in the first few weeks of life. Central nervous system involvement commonly follows the septicaemia and causes hyperaesthesia, neck rigidity and terminal paralysis. Because of the generally poor response to treatment, foals with polyarthritis frequently develop chronic arthritis and permanent joint damage.
Diagnosis and differential diagnosis
The diagnosis of S. equi infection relied upon the inoculation of blood agar containing colistin and nalidixic acid and overnight incubation at 37ºC in a 5 per cent CO2 atmosphere. β-haemolytic colonies of S. equi are inoculated into Todd Hewitt nutrient broth, which is incubated overnight at 37ºC in a 5 per cent CO2 atmosphere. Finally, these cultures are used to inoculate purple broth containing trehalose, lactose or sorbitol. Streptococcus equi does not ferment these sugars, whilst strains of S. zooepidemicus usually ferment lactose and sorbitol and Streptococcus dysgalactiae subspecies equisimilis (S. equisimilis), another common β-haemolytic streptococcus, ferments trehalose5. Therefore, the isolation and identification of S. equi is time-consuming and requires a minimum of 48 hours from receipt of clinical samples. This reporting delay provides an opportunity for S. equi to spread through naïve populations if potential cases are not isolated based on clinical signs alone. The detection of S. equi using the culture method is confounded by relatively poor sensitivity and the presence of other β-haemolytic bacteria, most notably S. zooepidemicus and S. equisimilis, which may lead to the reporting of false negative results in as many as 40 per cent of positive cases.70
Advances in polymerase chain reaction (PCR) technology have enabled this method to become the gold standard method for the detection of S. equi and diagnosis of strangles. Originally based on the detection of the SeM gene,61 current quantitative PCR (qPCR) formats detect seeI6 or a combination of eqbE and SEQ2190.70 This latter test also includes an internal control to provide quality assurance of negative results,70 whilst the former can be run in combination with a sodA qPCR control that detects S. zooepidemicus or S. equi.6 PCR assays can be completed within a few hours of sample receipt, providing a rapid, sensitive and specific means of detecting S. equi in clinical samples.
Endoscopic examination of the guttural pouches followed by qPCR of lavages is helpful in detecting clinically healthy long-term carriers of S. equi that shed only intermittently from the nose. Visual inspection of the pouches, removal of chondroids and the administration of topical antibiotics into the pouch can then be used to clear the persistent infection.65 Retesting guttural pouch lavages by qPCR that are taken two-weeks post-treatment confirms infection-free status.
SeM-specific antibodies may be measured by iELISA.54 Cross-reacting antibodies to conformational epitopes common to SeM and the SzM34 protein of S. zooepidemicus are removed by absorption of the serum or nasal wash with a suspension of heat-inactivated S. zooepidemicus.16, 54 However, this process, although successful in reducing assay background, has not been adopted in assays based on full length SeM. Convalescent SeM-specific serum antibody responses peak about five weeks after exposure to S. equi and remain elevated for at least six months.54
An iELISA assay using the N-terminal portion of SeM, which is unique to S. equi, has been developed to avoid cross-reactive responses to S. zooepidemicus.51 The test also incorporates the unique N-terminal domain of SEQ_2190 and has high sensitivity (93.3 per cent) and specificity (99.3 per cent).51 In addition to identifying horses that have been recently exposed to S. equi, the test also identifies antibody responses produced by persistently infected horses. Fourteen of 15 persistently infected horses, where their S. equi isolates had evidence of genome decay that suggested long-term carriage,26 tested positive using this assay. The iELISA is available in several countries around the world including the UK, France, Ireland, Australia and the United Arab Emirates. The strangles iELISA is a mandatory pre-import requirement when exporting horses to the United Arab Emirates and its wider use could greatly reduce the national and international transport of strangles to horses around the world.
Control
The very contagious nature of strangles requires that measures to control spread be rigorous and uncompromising. Infected animals must be identified and isolated as quickly as possible to minimize contagion, morbidity and disease severity.
The following guidelines for prevention are suggested:66
- Newly introduced animals, including nurse mares, should be isolated for three weeks and observed for signs of strangles.
- Care should be taken to ensure that equipment and personnel do not move between quarantined horses and those on the main yard.
- A blood sample taken from new arrivals can be used to identify recently exposed or persistently infected horses. If negative, a second sample taken two weeks later can identify horses that have seroconverted and may be incubating the infection. If positive, then the horse should be examined further by guttural pouch endoscopy and lavage, testing samples by qPCR. Carrier horses can then be treated, retested and confirmed to be free of S. equi infection before entering the main yard.
- Rectal temperatures should be taken daily during quarantine with a temperature of 38ºC or higher indicating the likely development of further clinical signs and shedding of S. equi.
- Horses without clinical signs of disease during the three-week quarantine period that test negative on serology are safe to enter the main yard.
The following guidelines for control are suggested:66
- Stop all movement onto and off the yard immediately following the identification of an index case. This should last at least three weeks post resolution of the last clinical case or persistent infection.
- Affected or presumptively infected horses should be immediately isolated and quarantined. Create three colour coded groups of horses, even if only separated by a double layer of electric fencing: the red group to contain all clinically affected horses; the amber group to include horses that had prior contact with clinically affected horses; and the green group to consist of horses with no known contact with affected horses.
- Equipment and tack should be labelled red/amber/green so as to prevent their inadvertent usage elsewhere.
- Rectal temperatures of horses in the green and amber groups should be measured twice daily.
- Febrile horses should be immediately moved to the red group.
- Clearly colour code buckets and drinking water. Disinfect water and buckets daily.
- If separate staff are not available, then staff should always move from green to amber to red groups and not back again.
- Testing of all horses in the amber and green groups’ post-resolution of the last clinical case using iELISA can be used to identify horses exposed to S. equi during the outbreak that only developed atypical strangles and persistently infected carriers.
- Screening clinically affected horses and those in the amber and green groups that were positive by iELISA by guttural pouch endoscopy and lavage should begin three weeks post-resolution of the last clinical signs. Positive horses should be treated and retested two weeks later before they are released back into the main yard and the yard reopens.
- If guttural pouch endoscopy and lavage is not an option, then nasopharyngeal swabs or washes should be tested by qPCR on three occasions at weekly intervals to identify persistently infected carriers.
- Only severely affected animals should be treated with antibiotics such as penicillin G, administered intramuscularly. Most cases recover uneventfully without antibiotic therapy and develop strong protective immune responses.
Vaccination
Horses generally have a solid immunity following recovery from strangles. In about 30 per cent of animals, however, this immunity does not persist and they become susceptible again a few months later.25, 44, 63 Passive colostral transfer involves mostly antibodies of the IgGb isotype, which distribute to the plasma and nasal secretions. Antibodies (IgA) in milk also contribute to nasopharyngeal protection during the first months of life.22
A purified M-protein antigen extract vaccine, StrepvaxII, is available in the United States. Naïve horses are given three doses at an interval of three weeks and an annual booster is required thereafter.20 However, the protection conferred by extract vaccines has been disappointing. One study suggested a reduction in the clinical attack rate of 50 per cent in vaccinates two weeks following the final vaccination.28 Adverse reactions include soreness or abscesses at injection sites and occasional cases of purpura hemorrhagica.28
An attenuated live, intranasal vaccine, Pinnacle IN, is available in the USA and some other territories. Two doses of the vaccine at a two- to three-week interval should be administered only to healthy animals. Annual booster doses are recommended. Following experimental challenge, nine out of 15 controls developed strangles compared with three out of 22 high dose (P = 0.0049) and two out of 22 low dose (P = 0.0023) vaccinates three weeks post V2.66 However, the vaccine can cause adverse reactions, which include clinical strangles.15 Indeed, the vaccine strain was recovered from 61 per cent of vaccinated horses that developed strangles.39
A live attenuated aroA deletion mutant of S. equi is available as a vaccine in Europe. Equilis StrepE, is administered submucosally on the inside of the upper lip.31 Immunity to experimental challenge persists for about three months. The vaccine lacks DIVA capability (Differentiating Infected from Vaccinated Animals). Painful reactions at injection sites may occur.31, 34 Bacterial replication of the vaccine strain has resulted in rare cases of clinical disease in vaccinated horses35 and an adverse reaction in a veterinarian following self-injection has also been reported.59
Alternative live attenuated vaccines are being developed. Whilst these vaccines confer excellent levels of protection, further improvements in their safety profile are required prior to commercialisation.50 A multicomponent subunit vaccine, Strangvac, is also in development in Sweden. The vaccine has an excellent safety profile, DIVA capability and early studies demonstrated good levels of protection in ponies, albeit shortly after final vaccination.24 The advances in our understanding of how S. equi causes disease provide an opportunity to develop safer and more effective vaccines against strangles. The administration of these vaccines to horses has the potential to induce immunity that confers protection against disease and may also help to reduce the proportion of horses that become persistently infected with S. equi. Such products, when used in combination with modern diagnostic tests, will have the potential to break the cycle of S. equi infection, dramatically reducing the number of strangles outbreaks over future years.
References
- ABBOT, E.L., SMITH, W.D., SIOU, G.P., CHIRIBOGA, C., SMITH, R.J., WILSON, J.A., HIRST, B.H. & KEHOE, M.A., 2007. Pili mediate specific adhesion of Streptococcus pyogenes to human tonsil and skin. Cellular Microbiology, 9, 1822-1833.
- ANZAI, T., KUWAMOTO, Y., WADA, R., SUGITA, S., KAKUDA, T., TAKAI, S., HIGUCHI, T. & TIMONEY, J.F., 2005. Variation in the N-terminal region of an M-like protein of Streptococcus equi and evaluation of its potential as a tool in epidemiologic studies. American Journal of Veterinary Research, 66, 2167-2171.
- ANZAI, T., TIMONEY, J.F., KUWAMOTO, Y., FUJITA, Y., WADA, R. & INOUE, T., 1999. In vivo pathogenicity and resistance to phagocytosis of Streptococcus equi strains with different levels of capsule expression. Veterinary Microbiology, 67, 277-286.
- ARTIUSHIN, S.C., TIMONEY, J.F., SHEORAN, A.S. & MUTHUPALANI, S.K., 2002. Characterization and immunogenicity of pyrogenic mitogens SePE-H and SePE-I of Streptococcus equi. Microbial Pathogenesis, 32, 71-85.
- BANNISTER, M.F., BENSON, C.E. & SWEENEY, C.R., 1985. Rapid species identification of group C streptococci isolated from horses. Journal of Clinical Microbiology, 21, 524-526.
- BAVERUD, V., JOHANSSON, S.K. & ASPAN, A., 2007. Real-time PCR for detection and differentiation of Streptococcus equi subspecies equi and Streptococcus equi subsp. zooepidemicus. Veterinary Microbiology, 124, 219-229.
- BEARDEN, S.W., FETHERSTON, J.D. & PERRY, R.D., 1997. Genetic organization of the yersiniabactin biosynthetic region and construction of avirulent mutants in Yersinia pestis. Infection and Immunity, 65, 1659-1668.
- BERES, S.B., SESSO, R., PINTO, S.W., HOE, N.P., PORCELLA, S.F., DELEO, F.R. & MUSSER, J.M., 2008. Genome sequence of a lancefield group C Streptococcus zooepidemicus strain causing epidemic nephritis: new information about an old disease. PLoS (Public Library of Science) One, 3, e3026.
- BERLIN, D., KELMER, G., STEINMAN, A. & SUTTON, G.A., 2013. Successful medical management of intra-abdominal abscesses in 4 adult horses. The Canadian Veterinary Journal, 54, 157-161.
- BIGGERS, J.C. & INGRAM, P.L., 1948. Studies on equine purpura haemorrhagica. The British Veterinary Journal, 104, 214-221.
- BJORNSDOTTIR, S., HARRIS, S.R., SVANSSON, V., GUNNARSSON, E., SIGURETHARDOTTIR, O.G., GAMMELJORD, K., STEWARD, K.F., NEWTON, J.R., ROBINSON, C., CHARBONNEAU, A.R.L., PARKHILL, J., HOLDEN, M.T.G. & WALLER, A.S., 2017. Genomic dissection of an Icelandic epidemic of respiratory disease in horses and associated zoonotic cases. MBio (American Society for Microbiology), 8.
- BOSCHWITZ, J.S. & TIMONEY, J.F., 1994. Characterization of the antiphagocytic activity of equine fibrinogen for Streptococcus equi subspecies equi. Microbial Pathogenesis, 17, 121-129.
- BOSCHWITZ, J.S. & TIMONEY, J.F., 1994. Inhibition of C3 deposition on Streptococcus equi subspecies equi by M protein: a mechanism for survival in equine blood. Infection and Immunity, 62, 3515-3520.
- CHANTER, N., TALBOT, N.C., NEWTON, J.R., HEWSON, D. & VERHEYEN, K., 2000. Streptococcus equi with truncated M-proteins isolated from outwardly healthy horses. Microbiology, 146 (Pt 6), 1361-1369.
- CURSONS, R., PATTY, O., STEWARD, K.F. & WALLER, A.S., 2015. Strangles in horses can be caused by vaccination with Pinnacle I. N. Vaccine, 33, 3440-3443.
- DAVIDSON, A., TRAUB-DARGATZ, J.L., MAGNUSON, R., HILL, A., IRWIN, V., NEWTON, R., WALLER, A., SMITH, K., CALLAN, R.J., MEEHAN, M., OWEN, P. & SALMAN, M., 2008. Lack of correlation between antibody titers to fibrinogen-binding protein of Streptococcus equi and persistent carriers of strangles. Journal of Veterinary Diagnostic Investigation, 20, 457-462.
- FALLON, E.H., 1969. The clinical aspects of streptococcic infections of horses. Journal of the American Veterinary Medical Association, 155, 413-414.
- FLANAGAN, J., COLLIN, N., TIMONEY, J., MITCHELL, T., MUMFORD, J.A. & CHANTER, N., 1998. Characterization of the haemolytic activity of Streptococcus equi. Microbial Pathogenesis, 24, 211-221.
- GALAN, J.E. & TIMONEY, J.F., 1985. Immune complexes in purpura hemorrhagica of the horse contain IgA and M antigen of Streptococcus equi. Journal of Immunology, 135, 3134-3137.
- GALAN, J.E. & TIMONEY, J.F., 1987. Molecular analysis of the M protein of Streptococcus equi and cloning and expression of the M protein gene in Escherichia coli. Infection and Immunity, 55, 3181-3187.
- GALAN, J.E. & TIMONEY, J.F., 1988. Immunologic and genetic comparison of Streptococcus equi isolates from the United States and Europe. Journal of Clinical Microbiology, 26, 1142-1146.
- GALAN, J.E., TIMONEY, J.F. & LENGEMANN, F.W., 1986. Passive transfer of mucosal antibody to Streptococcus equi in the foal. Infection and Immunity, 54, 202-206.
- GEORGE, J.L., REIF, J.S., SHIDELER, R.K., SMALL, C.J., ELLIS, R.P., SNYDER, S.P. & MCCHESNEY, A.E., 1983. Identification of carriers of Streptococcus equi in a naturally infected herd. Journal of the American Veterinary Medical Association, 183, 80-84.
- GUSS, B., FLOCK, M., FRYKBERG, L., WALLER, A.S., ROBINSON, C., SMITH, K.C. & FLOCK, J.I., 2009. Getting to grips with strangles: an effective multi-component recombinant vaccine for the protection of horses from Streptococcus equi infection. PLoS (Public Library of Science) Pathogens, 5, e1000584.
- HAMLEN, H.J.T., J.F., BELL, R.J., 1992. Haematologic parameters of foals during a strangles epizootic. Equine Veterinary Science, 12, 86-92.
- HARRIS, S.R., ROBINSON, C., STEWARD, K.F., WEBB, K.S., PAILLOT, R., PARKHILL, J., HOLDEN, M.T. & WALLER, A.S., 2015. Genome specialization and decay of the strangles pathogen, Streptococcus equi, is driven by persistent infection. Genome Research, 25, 1360-1371.
- HEATHER, Z., HOLDEN, M.T., STEWARD, K.F., PARKHILL, J., SONG, L., CHALLIS, G.L., ROBINSON, C., DAVIS-POYNTER, N. & WALLER, A.S., 2008. A novel streptococcal integrative conjugative element involved in iron acquisition. Molecular Microbiology, 70, 1274-1292.
- HOFFMAN, A.M., STAEMPFLI, H.R., PRESCOTT, J.F. & VIEL, L., 1991. Field evaluation of a commercial M-protein vaccine against Streptococcus equi infection in foals. American Journal of Veterinary Research, 52, 589-592.
- HOLDEN, M.T., HEATHER, Z., PAILLOT, R., STEWARD, K.F., WEBB, K., AINSLIE, F., JOURDAN, T., BASON, N.C., HOLROYD, N.E., MUNGALL, K., QUAIL, M.A., SANDERS, M., SIMMONDS, M., WILLEY, D., BROOKS, K., AANENSEN, D.M., SPRATT, B.G., JOLLEY, K.A., MAIDEN, M.C., KEHOE, M., CHANTER, N., BENTLEY, S.D., ROBINSON, C., MASKELL, D.J., PARKHILL, J. & WALLER, A.S., 2009. Genomic evidence for the evolution of Streptococcus equi: host restriction, increased virulence, and genetic exchange with human pathogens. PLoS (Public Library of Science) Pathogens, 5, e1000346.
- IVENS, P.A., MATTHEWS, D., WEBB, K., NEWTON, J.R., STEWARD, K., WALLER, A.S., ROBINSON, C. & SLATER, J.D., 2011. Molecular characterisation of 'strangles' outbreaks in the UK: the use of M-protein typing of Streptococcus equi subspecies equi. Equine Veterinary Journal, 43, 359-364.
- JACOBS, A.A., GOOVAERTS, D., NUIJTEN, P.J., THEELEN, R.P., HARTFORD, O.M. & FOSTER, T.J., 2000. Investigations towards an efficacious and safe strangles vaccine: submucosal vaccination with a live attenuated Streptococcus equi. Veterinary Record, 147, 563-567.
- JORM, L.R., 1990. Strangles in horse studs: incidence, risk factors and effect of vaccination. Australian Veterinary Journal, 67, 436-439.
- JORM, L.R., LOVE, D.N., BAILEY, G.D., MCKAY, G.M. & BRISCOE, D.A., 1994. Genetic structure of populations of beta-haemolytic Lancefield group C streptococci from horses and their association with disease. Research in Veterinary Science, 57, 292-299.
- KELLY, C., BUGG, M., ROBINSON, C., MITCHELL, Z., DAVIS-POYNTER, N., NEWTON, J.R., JOLLEY, K.A., MAIDEN, M.C. & WALLER, A.S., 2006. Sequence variation of the SeM gene of Streptococcus equi allows discrimination of the source of strangles outbreaks. Journal of Clinical Microbiology, 44, 480-486.
- KEMP-SYMONDS, J., KEMBLE, T. & WALLER, A., 2007. Modified live Streptococcus equi ('strangles') vaccination followed by clinically adverse reactions associated with bacterial replication. Equine Veterinary Journal, 39, 284-286.
- LANNERGARD, J., FRYKBERG, L. & GUSS, B., 2003. CNE, a collagen-binding protein of Streptococcus equi. FEMS Microbiology Letters, 222, 69-74.
- LEWIS, M.J., MEEHAN, M., OWEN, P. & WOOF, J.M., 2008. A common theme in interaction of bacterial immunoglobulin-binding proteins with immunoglobulins illustrated in the equine system. Journal of Biological Chemistry, 283, 17615-17623.
- LINDSAY, A.M., ZHANG, M., MITCHELL, Z., HOLDEN, M.T., WALLER, A.S., SUTCLIFFE, I.C. & BLACK, G.W., 2009. The Streptococcus equi prophage-encoded protein SEQ2045 is a hyaluronan-specific hyaluronate lyase that is produced during equine infection. Microbiology, 155, 443-449.
- LIVENGOOD, J.L., LANKA, S., MADDOX, C. & TEWARI, D., 2016. Detection and differentiation of wild-type and a vaccine strain of Streptococcus equi subspecies equi using pyrosequencing. Vaccine, 34, 3935-3937.
- LOPEZ-ALVAREZ, M.R., SALZE, M., CENIER, A., ROBINSON, C., PAILLOT, R. & WALLER, A.S., 2017. Immunogenicity of phospholipase A2 toxins and their role in Streptococcus equi pathogenicity. Veterinary Microbiology, 204, 15-19.
- MCLEAN, R., RASH, N.L., ROBINSON, C., WALLER, A.S. & PAILLOT, R., 2015. Localised mitogenic activity in horses following infection with Streptococcus equi. Research in Veterinary Science, 100, 100-104.
- MEEHAN, M., LYNAGH, Y., WOODS, C. & OWEN, P., 2001. The fibrinogen-binding protein (FgBP) of Streptococcus equi subspecies equi additionally binds IgG and contributes to virulence in a mouse model. Microbiology, 147, 3311-3322.
- MUHKTAR, M.M. & TIMONEY, J.F., 1988. Chemotactic response of equine polymorphonuclear leucocytes to Streptococcus equi. Research in Veterinary Science, 45, 225-229.
- NARA, P.L., KRAKOWKA, S., POWERS, T.E. & GARG, R.C., 1983. Experimental Streptococcus equi infection in the horse: correlation with in vivo and in vitro immune responses. American Journal of Veterinary Research, 44, 529-534.
- NEWTON, J.R., WOOD, J.L., DUNN, K.A., DEBRAUWERE, M.N. & CHANTER, N., 1997. Naturally occurring persistent and asymptomatic infection of the guttural pouches of horses with Streptococcus equi. Veterinary Record, 140, 84-90.
- PAILLOT, R., ROBINSON, C., STEWARD, K., WRIGHT, N., JOURDAN, T., BUTCHER, N., HEATHER, Z. & WALLER, A.S., 2010. Contribution of each of four Superantigens to Streptococcus equi-induced mitogenicity, gamma interferon synthesis, and immunity. Infection and Immunity, 78, 1728-1739.
- POINTON, J.A., SMITH, W.D., SAALBACH, G., CROW, A., KEHOE, M.A. & BANFIELD, M.J., 2010. A highly unusual thioester bond in a pilus adhesin is required for efficient host cell interaction. The Journal of Biological Chemistry, 285, 33858-33866.
- PUSTERLA, N., WATSON, J.L., AFFOLTER, V.K., MAGDESIAN, K.G., WILSON, W.D. & CARLSON, G.P., 2003. Purpura haemorrhagica in 53 horses. Veterinary Record, 153, 118-121.
- PUSTERLA, N., WHITCOMB, M.B. & WILSON, W.D., 2007. Internal abdominal abscesses caused by Streptococcus equi subspecies equi in 10 horses in California between 1989 and 2004. Veterinary Record, 160, 589-592.
- ROBINSON, C., HEATHER, Z., SLATER, J., POTTS, N., STEWARD, K.F., MASKELL, D.J., FONTAINE, M.C., LEE, J.J., SMITH, K. & WALLER, A.S., 2015. Vaccination with a live multi-gene deletion strain protects horses against virulent challenge with Streptococcus equi. Vaccine, 33, 1160-1167.
- ROBINSON, C., STEWARD, K.F., POTTS, N., BARKER, C., HAMMOND, T.A., PIERCE, K., GUNNARSSON, E., SVANSSON, V., SLATER, J., NEWTON, J.R. & WALLER, A.S., 2013. Combining two serological assays optimises sensitivity and specificity for the identification of Streptococcus equi subspecies equi exposure. Veterinary Journal, 197, 188-191.
- RUFUS, J. (ed.) 1251. De Medicina Equorum.
- SCHUTZ, J.W., 1888. The Streptococcus of Strangles. The Journal of Comparative Pathology and Therapeutics, 1, 191 - 208.
- SHEORAN, A.S., SPONSELLER, B.T., HOLMES, M.A. & TIMONEY, J.F., 1997. Serum and mucosal antibody isotype responses to M-like protein (SeM) of Streptococcus equi in convalescent and vaccinated horses. Veterinary Immunology Immunopathology, 59, 239-251.
- STEWARD, K.F., ROBINSON, C., MASKELL, D.J., NENCI, C. & WALLER, A.S., 2017. Investigation of the Fim1 putative pilus locus of Streptococcus equi subspecies equi. Microbiology.
- SWEENEY, C.R., TIMONEY, J.F., NEWTON, J.R. & HINES, M.T., 2005. Streptococcus equi infections in horses: guidelines for treatment, control, and prevention of strangles. Journal of Veterinary Internal Medicine, 19, 123-134.
- SWEENEY, C.R., WHITLOCK, R.H., MEIRS, D.A., WHITEHEAD, S.C. & BARNINGHAM, S.O., 1987. Complications associated with Streptococcus equi infection on a horse farm. Journal of the American Veterinary Medical Association, 191, 1446-1448.
- THEILER, A., 1918. Observations on an epizootic contagious catarrh of the respiratory organs of equines and its relation to purpura haemorrhagica. In Seventh and eight reports of the Director of Veterinary Services, 361-393 (Department of Agriculture, Union of South Africa).
- THOMPSON, R.N. & MCNICHOLL, B.P., 2010. Needlestick and infection with horse vaccine. BMJ Case Reports, 2010,
- TIMONEY, J.F., 1993. Strangles. Veterinary Clinics of North America: Equine Practice, 9, 365-374.
- TIMONEY, J.F. & ARTIUSHIN, S.C., 1997. Detection of Streptococcus equi in equine nasal swabs and washes by DNA amplification. Veterinary Record, 141, 446-447.
- TIMONEY, J.F. & KUMAR, P., 2008. Early pathogenesis of equine Streptococcus equi infection (strangles). Equine Veterinary Journal, 40, 637-642.
- TODD, A.G., 1910. Strangles. Journal of Comparative Pathology Therapy, 23, 212-229.
- VAN DE RIJN, I. & KESSLER, R.E., 1980. Growth characteristics of group A streptococci in a new chemically defined medium. Infection and Immunity, 27, 444-448.
- VERHEYEN, K., NEWTON, J.R., TALBOT, N.C., DE BRAUWERE, M.N. & CHANTER, N., 2000. Elimination of guttural pouch infection and inflammation in asymptomatic carriers of Streptococcus equi. Equine Veterinary Journal, 32, 527-532.
- WALLER, A.S., 2014. New perspectives for the diagnosis, control, treatment, and prevention of strangles in horses. Veterinary Clinics of North America: Equine Practice, 30, 591-607.
- WALLER, A.S., 2016. Strangles: a pathogenic legacy of the war horse. Veterinary Record, 178, 91-92.
- WALLER, A.S., PAILLOT, R. & TIMONEY, J.F., 2011. Streptococcus equi: a pathogen restricted to one host. Journal of Medical Microbiology, 60, 1231-1240.
- WALLER, A.S. & ROBINSON, C., 2013. Streptococcus zooepidemicus and Streptococcus equi evolution: the role of CRISPRs. Biochemical Society Transactions, 41, 1437-1443.
- WEBB, K., BARKER, C., HARRISON, T., HEATHER, Z., STEWARD, K.F., ROBINSON, C., NEWTON, J.R. & WALLER, A.S., 2013. Detection of Streptococcus equi subspecies equi using a triplex qPCR assay. Veterinary Journal, 195, 300-304.
- WEBB, K., JOLLEY, K.A., MITCHELL, Z., ROBINSON, C., NEWTON, J.R., MAIDEN, M.C. & WALLER, A., 2008. Development of an unambiguous and discriminatory multilocus sequence typing scheme for the Streptococcus zooepidemicus group. Microbiology, 154, 3016-3024.
- WISECUP, W.G., SCHRODER, C. & PAGE, N.P., 1967. Isolation of Streptococcus equi from burros. Journal of the American Veterinary Medical Association, 150, 303-306.




